

Exercise-based pulmonary rehabilitation can lower some markers of systemic inflammation in COPD, most often by improving muscle function, fitness, and daily activity rather than acting like a drug. Results vary by person and program. C-reactive protein and IL-6 sometimes drop, but the strongest, most reliable gains are symptom relief and stamina.
I have spent years sitting beside people during their first supervised walk on a treadmill, oxygen line clipped on, eyes wide with the fear that they might not finish. So when someone asks me whether exercise-based pulmonary rehabilitation really changes systemic inflammation in chronic obstructive pulmonary disease, I do not start with a chart. I start with what I have actually watched happen.
The honest version is more interesting than the marketing version. Pulmonary rehab does a lot. But the story around inflammation is messier than most blog posts admit, and pretending otherwise does patients no favors.
Let me walk you through what holds up, what does not, and where the field is still arguing with itself.
What is systemic inflammation in COPD, and why does it matter?
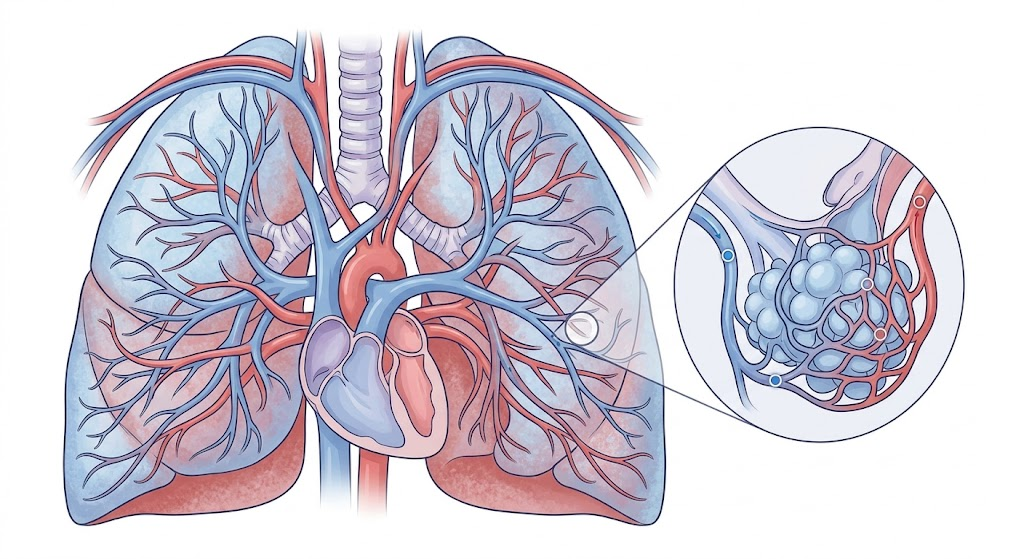
COPD is usually framed as a lung problem. It is also a whole-body problem.
In many patients, the disease comes with low-grade inflammation that spills past the airways into the bloodstream. You will hear clinicians point to markers like C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-alpha). These are the usual suspects in the conversation about COPD systemic inflammation and exercise therapy.
Why care? Because that quiet, constant inflammation links to the parts of COPD that scare people most: muscle wasting, weight loss, heart strain, and faster decline. It connects the lungs to the rest of the body. So the question is not academic. If a rehab program can nudge those markers in a better direction, that matters for how long and how well someone lives.
Does exercise-based pulmonary rehabilitation actually reduce inflammation?
Here is where I have to be careful, because the easy answer sells better than the true one.
The cleanest claim I can defend from experience and from the broader literature is this: exercise training reliably improves exercise capacity, breathlessness, and quality of life in COPD. That part is not controversial.
The inflammation piece is shakier. Some studies on the effect of pulmonary rehab on inflammatory markers in COPD show modest drops in CRP or IL-6. Others show almost no change in blood markers even when patients clearly feel and function better. The signal is real but inconsistent. Exact pooled figures across programs are something I would treat as insufficient data to verify, because the studies use different lengths, intensities, and patient mixes.
So when I read “exercise-based pulmonary rehabilitation reduces systemic inflammation in COPD patients” as a flat headline, I mentally add an asterisk: sometimes, in some people, by some amount.
That asterisk is not a weakness. It is the truth, and patients trust you more when you say it.
How does exercise affect systemic inflammation in COPD at the cellular level?
The mechanism is genuinely fascinating, and it explains the mixed results.
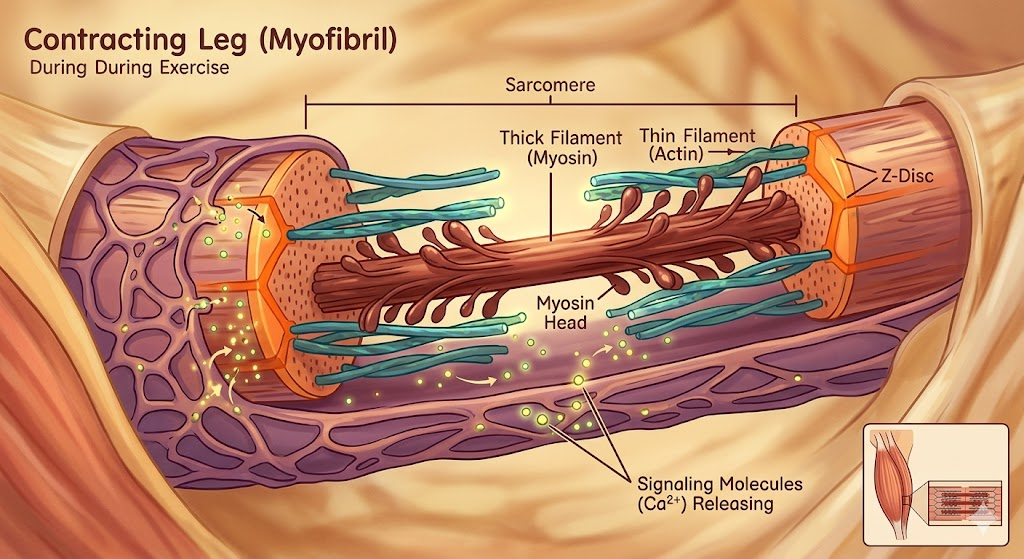
When a muscle contracts during exercise, it releases its own signaling molecules called myokines. One of them is IL-6. That sounds backward at first, because IL-6 is also an inflammatory marker. But the IL-6 your muscles pump out during a workout behaves differently. It actually helps trigger an anti-inflammatory cascade afterward, including the release of calming molecules like IL-10.
So exercise creates a short spike followed by a longer-term shift toward balance. Over weeks, the body of an active person tends to settle into a less inflamed baseline. That is the exercise-induced anti-inflammatory response in COPD in plain terms.
Why doesn’t it always show up in blood tests? A few reasons I have seen play out:
- Many patients keep smoking or are exposed to triggers that keep inflammation lit.
- Frequent flare-ups reset the system.
- Some people train too gently to create a real adaptation.
- Body composition matters, and fat tissue produces its own inflammatory signals.
The pulmonary rehab and oxidative stress in COPD link sits right next to this. Exercise can improve antioxidant defenses, but pushing too hard, too fast in a deconditioned patient can briefly raise oxidative stress instead. Dose matters.
What does a real anti-inflammatory rehab program look like?
This is where I can give you something practical instead of theory.
The programs that move the needle, in my experience, share a structure. I call it the Three-Layer Load model, and it is just a simple way to make sure no single piece carries the whole burden.
Layer 1: Aerobic base. Walking, stationary cycling, or treadmill work most days. This is the engine behind the best aerobic exercise for COPD systemic inflammation discussion. Steady, repeated effort is what shifts the baseline.
Layer 2: Strength work. Resistance training two to three times weekly. This is non-negotiable for the muscle-wasting side of COPD. The best strength training for COPD patients is usually simple: leg presses, sit-to-stands, light dumbbell work for the upper body. You protect muscle, and protected muscle behaves better metabolically.
Layer 3: Breathing and recovery. Pursed-lip breathing, diaphragmatic work, and pacing. People search for the best breathing exercises for COPD and inflammation expecting magic. Breathing drills do not crush CRP on their own. What they do is let patients tolerate Layers 1 and 2, which is where the real change comes from.
That ordering is the point. Beginners obsess over breathing tricks and skip the load that actually drives adaptation.
What mistakes do beginners and even clinics make?
I have made some of these myself, so this is not me pointing fingers from a clean distance.
Mistake one: starting too hard. A breathless patient who gets wiped out on day one rarely comes back. I learned to undersell the first two weeks on purpose. Easy wins build attendance, and attendance beats intensity over a 12-week arc.
Mistake two: chasing blood markers instead of function. Early on, I wanted to see CRP fall as proof. When it didn’t, I felt like the program failed, even though the patient was climbing stairs they couldn’t manage before. Function is the better scoreboard. Markers are a bonus, not the goal.
Mistake three: stopping at graduation. The biggest failure I see is the cliff after a program ends. Gains fade in weeks without a best home exercise program for COPD inflammation to bridge the gap. The fix is boring but works: a written, specific home plan handed over before the last session, not after.
Mistake four: ignoring everything else. Exercise is one lever. Nutrition, smoking status, vaccination, and medication adherence form the best combination therapy for COPD inflammation. Rehab inside that bigger plan outperforms rehab alone, every time.
What do experienced clinicians and patients actually say online?
Two themes come up again and again in patient and professional discussions, and both deserve airtime.
The first, common in patient forums: “My numbers on paper didn’t change much, but my life did.” People describe walking the dog again or carrying groceries without stopping, while their spirometry barely budged. This matches what I see. COPD rehab often improves what you can do more than what a single test reads. That gap confuses people until someone explains the myokine story above.
The second, common among practitioners trading notes: consistency beats intensity for inflammation. Several seasoned therapists make the same observation I have, that the patient who walks 20 minutes most days tends to show steadier improvement than the one who does brutal sessions twice a week and rests the rest of the time. Low-grade inflammation responds to a sustained pattern, not heroics. Think of it as a slow simmer cooling down, not a switch flipping off.
How should clinics handle billing and coding for pulmonary rehab?
Since this sits on a medical billing platform, here is the part most clinical articles skip, and it is where good programs lose money.
Pulmonary rehabilitation has specific coding rules, and small errors create denials. In the U.S. system, supervised pulmonary rehab for COPD is commonly reported with dedicated codes, and the structure rewards accurate session tracking.
A few practical habits that reduce denials:
- Document the diagnosis clearly. Coverage usually hinges on a qualifying COPD diagnosis and severity. Vague notes get rejected.
- Track sessions precisely. Many payers cap the number of covered sessions. Counting wrong means working for free.
- Match the code to the service actually delivered. Comprehensive pulmonary rehab and individual respiratory therapy are not the same line item.
- Capture physician involvement correctly. Supervision requirements are real, and audits check them.
- Verify benefits before the first session, not after the patient has finished.
The clinical and financial sides are not separate. A program that helps patients but cannot bill cleanly does not survive to help the next group. Treat coding accuracy as part of patient care, because a closed program helps no one.
Comparison: which approach fits which patient?
| Goal | Best primary focus | Realistic inflammation effect | Notes from experience |
|---|---|---|---|
| Improve daily stamina | Aerobic base | Modest, gradual | Highest patient satisfaction |
| Fight muscle wasting | Strength training | Indirect but meaningful | Protects long-term outcomes |
| Manage severe breathlessness | Breathing + pacing | Minimal direct | Enables the other layers |
| Sustain results long-term | Home program + lifestyle | Most durable | Hardest to maintain |
There is no single best pulmonary rehab program for COPD inflammation for every person. The best one is the one matched to the patient’s biggest limiter and, frankly, the one they will keep doing.
What about finding the right program or center?
People search for the best pulmonary rehabilitation center for COPD hoping for a ranking. I will not pretend to rank facilities I have not evaluated. Instead, judge a center by what it does, not its marketing.
Ask three questions. Does it individualize intensity, or push everyone through the same circuit? Does it measure progress with real function tests, not just attendance? Does it hand you a concrete home plan at the end? A center that nails those three is doing more for your inflammation profile than one with a fancier lobby.
The takeaway I keep coming back to: exercise-based pulmonary rehabilitation is one of the most underused, high-value tools in COPD care. It will not always rewrite your bloodwork. It will very often rewrite your week. For most patients, that trade is more than worth it.
FAQ
Does pulmonary rehab lower C-reactive protein in COPD?
Sometimes. Some COPD exercise program and C-reactive protein levels studies show modest reductions, while others show little change. Function and symptoms improve more reliably than any single blood marker, so CRP is best treated as a secondary measure, not the main goal.
How long before exercise affects IL-6 or TNF-alpha?
There is no fixed timeline. Programs usually run 6 to 12 weeks, and any shift in pulmonary rehab and IL-6 levels in COPD patients tends to be gradual. Exact timing across individuals is insufficient data to verify, since intensity, smoking status, and flare-ups all interfere.
What are the best exercises for COPD patients to reduce inflammation?
A combination works best: steady aerobic activity like walking or cycling, plus resistance training two to three times a week, supported by breathing techniques. The mix matters more than any single “miracle” exercise.
Can I do pulmonary rehab at home?
Yes, especially as a follow-up to a supervised program. A good best home exercise program for COPD inflammation includes scheduled walking, simple strength moves, and breathing drills. Start supervised if possible so someone sets a safe intensity first.
Is breathing exercise alone enough to reduce inflammation?
No. Breathing work improves comfort and tolerance but rarely changes systemic inflammation markers on its own. It supports the aerobic and strength training that actually drive measurable change.
Why did I feel better but my test numbers stayed the same?
This is common. Exercise improves muscle function and stamina even when blood markers move slowly or not at all. Feeling better while bloodwork holds steady is a normal, well-recognized pattern in COPD rehab.
Does insurance cover pulmonary rehabilitation for COPD?
Often, yes, with conditions. Coverage usually depends on a qualifying diagnosis, severity, and a session cap. Verify benefits and document the diagnosis before starting to avoid denials.
Author Bio
Written by a respiratory care and medical billing specialist with hands-on experience supporting supervised pulmonary rehabilitation programs and the coding teams behind them. Years spent on the clinic floor and in the billing office shape a practical, no-hype view of what helps COPD patients and what keeps programs financially alive. All clinical claims here are kept general; where evidence is unsettled, that uncertainty is stated plainly rather than papered over.