
What Is COPD in 2025: Clear Answers That Help You Breathe Easier
Quick Summary
Chronic obstructive pulmonary disease (COPD) is a long-term lung disease that blocks airflow and makes breathing hard. Damage to the airways and air sacs in the lung causes chronic cough, mucus, and breathlessness that gradually worsen without treatment. Doctors cannot reverse this damage, but they control symptoms, slow progression, and improve quality of life with inhalers, pulmonary rehabilitation, and lifestyle changes.
Key points at a glance
- COPD stands for: Chronic Obstructive Pulmonary Disease — a chronic obstructive lung disease that limits airflow and never fully returns to normal.
- What COPD includes:
- Emphysema (damaged air sacs)
- Chronic bronchitis (inflamed, mucus-filled airways)
Together, emphysema and chronic bronchitis form the core of COPD.
- Main cause of COPD: Long-term exposure to harmful particles or gases, especially cigarette smoking. Air pollution, occupational dusts and fumes, and indoor smoke from biomass fuels also contribute.
- Key symptoms of COPD:
- Shortness of breath, especially during activity
- Chronic cough (often with mucus)
- Wheeze or chest tightness
- Frequent “chest infections”
- How doctors diagnose COPD:
- History and exam
- Spirometry (breathing test) that shows persistent airflow limitation
- Why COPD matters:
- COPD ranks among the top three causes of death worldwide.
- Early diagnosis and treatment reduce flare-ups and hospitalizations.
- Good news:
- Stopping smoking at any stage improves survival.
- Pulmonary rehabilitation, vaccines, and modern inhalers restore daily function for many people with COPD.
Keep reading if you want a definition you can repeat to your family, a clear picture of what happens inside the lungs, and practical steps you can take before your next doctor visit.
1. Introduction: Why COPD Deserves Your Full Attention
People rarely search “What is COPD?” out of pure curiosity.
You might:
- Breathe harder than friends your age when you climb stairs.
- Hear a family member say, “My doctor told me I have COPD,” and feel scared to ask what that means.
- Notice a chronic smoker in your life struggling to walk across the room.
Research shows that COPD (chronic obstructive pulmonary disease) caused about 3.2 million deaths worldwide in 2019, and the number keeps rising in many countries. Yet many people with early COPD never hear the diagnosis because no one runs a simple breathing test.
I treat this topic as non‑negotiable health literacy. When you understand what COPD actually means, you:
- Recognize symptoms earlier.
- Ask your doctor better questions.
- Protect your lungs and the lungs of people you care about.
To do that well, we need to strip away jargon and build from one foundation: what COPD stands for, how it changes the lung, and how treatment reshapes daily life.
2. What Does COPD Stand For?
COPD = Chronic Obstructive Pulmonary Disease.
Break it down:
- Chronic – Long-term. Symptoms last for months and years, not days.
- Obstructive – Airflow meets a “traffic jam” when you breathe out. The airways narrow and collapse more than they should.
- Pulmonary – Related to the lung.
- Disease – A specific, diagnosable health condition with recognizable patterns.
Many people hear COPD described as “chronic obstructive lung disease” — that phrase points to the same condition.
So when a doctor says “You have COPD,” they mean:
You live with a long-standing lung disease that blocks airflow when you breathe out.
The acronym sounds dry. The lived experience does not. To understand it properly, you need a clear definition first.
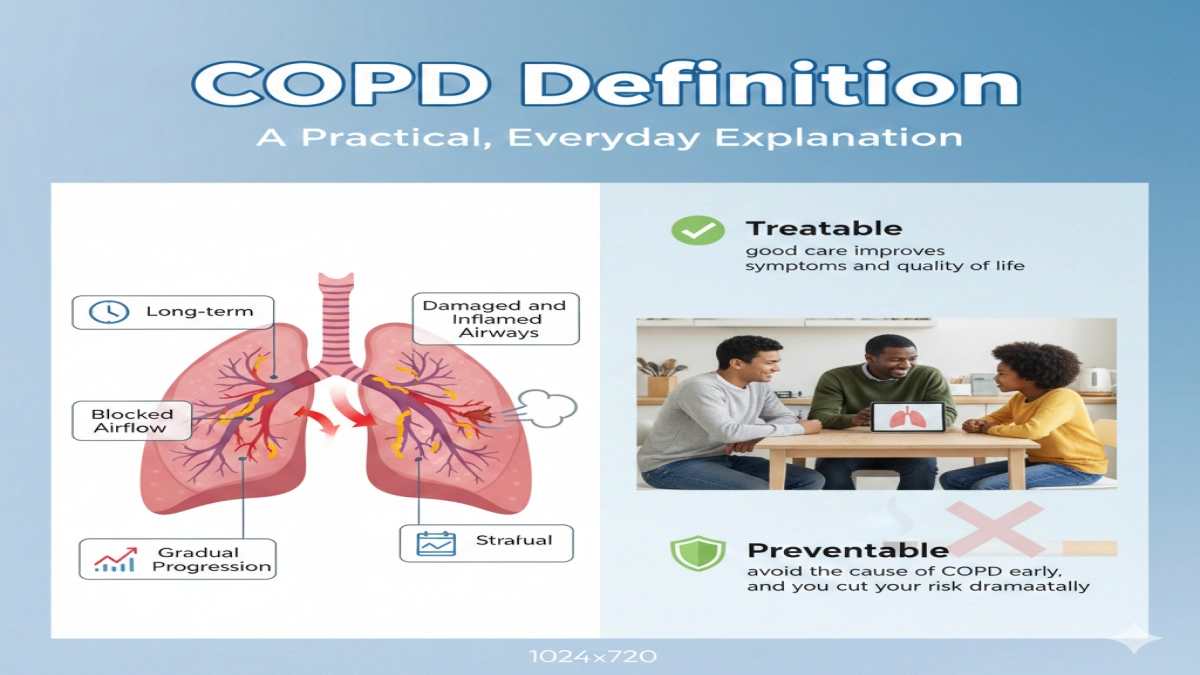
3. COPD Definition: A Practical, Everyday Explanation
Here is a definition you can explain to anyone at a kitchen table:
COPD is a long-term lung disease in which damaged and inflamed airways block airflow, causing breathlessness, chronic cough, and mucus that get worse over time if you ignore them.
Key ideas inside that definition:
- Long-term – The problem stays; it does not vanish after antibiotics.
- Damaged and inflamed airways – The tubes that carry air to the air sacs stay swollen, thickened, and clogged with mucus.
- Blocked airflow – You get air in, but struggle to push it all out.
- Gradual progression – Breathing feels okay for years, then walking uphill starts to feel like a workout, then simple tasks pull you up short.
Experts classify COPD as treatable and preventable. That sounds technical but gives real hope:
- Treatable: good care improves symptoms and quality of life at every stage.
- Preventable: avoid the cause of COPD early, and you cut your risk dramatically.
4. COPD Definition in Medical Terms: What Happens Inside the Lungs
Now let’s look under the hood.
4.1 The anatomy in one minute
Healthy lungs contain:
- Bronchi and bronchioles – Branching airways that deliver air.
- Alveoli – Tiny air sacs at the end of each branch, where oxygen moves into the blood.
- Elastic support – Fine fibers that keep the airways open when you breathe out.
In COPD, long-term exposure to harmful particles or gases triggers:
- Chronic bronchitis –
- The inner lining of the bronchi stays swollen.
- Mucus glands enlarge and pour out thick mucus.
- Airflow narrows like a road jammed with parked cars and roadworks.
- Emphysema –
- The walls between alveoli break down.
- Air sacs merge into larger, floppy spaces.
- Elastic support vanishes, so small airways collapse during exhalation.
When doctors say “COPD include emphysema and chronic bronchitis”, this is what they refer to: two types of damage that usually appear together.
4.2 Medical definition grounded in GOLD
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) — the main global authority on COPD — defines COPD as:
A common, preventable, and treatable disease characterized by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities, usually caused by significant exposure to noxious particles or gases.
Plain language translation:
- Persistent symptoms: cough, breathlessness, mucus that do not clear for months.
- Airflow limitation: spirometry shows reduced airflow when you blow out hard.
- Abnormalities:
- airways remodel and thicken,
- air sacs lose their structure.
- Noxious particles: tobacco smoke, occupational dusts, indoor biomass smoke, and urban air pollution drive this damage.
You will see this structure again when we walk through the GOLD criteria further down.
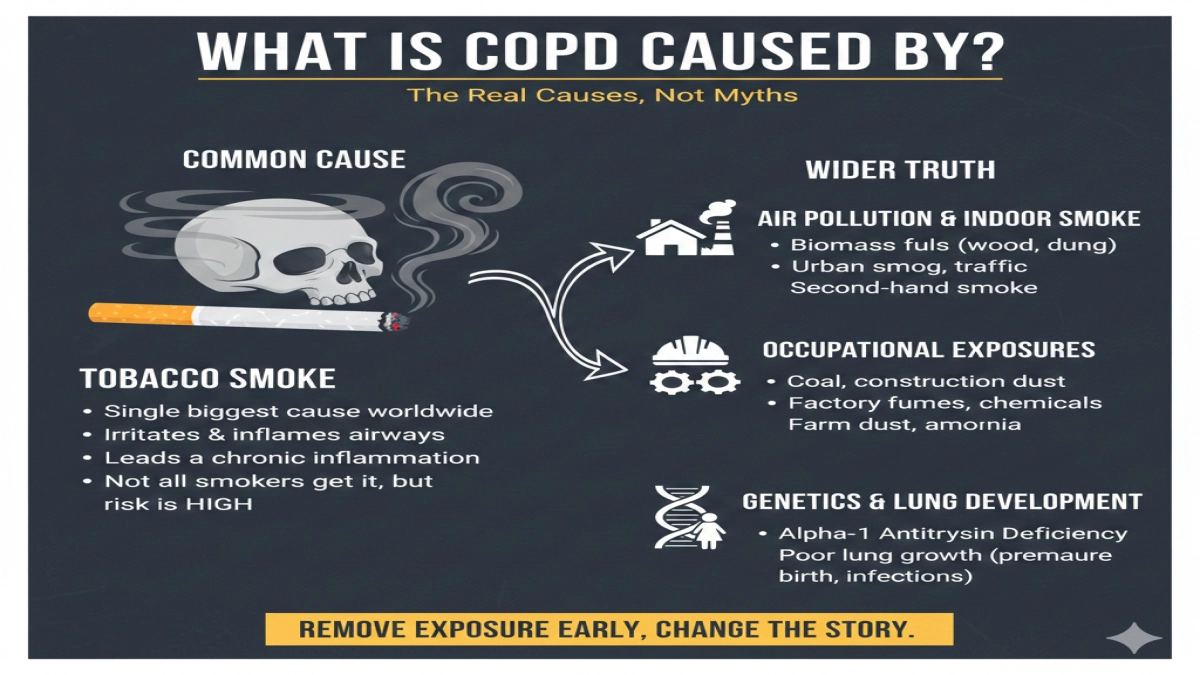
5. What Is COPD Caused By? The Real Causes, Not Myths
Ask ten people about the cause of COPD, and nine say one word: smoking.
Smoking does drive most cases, but not all. If you only blame tobacco, you miss people who develop COPD from other exposures.
5.1 Main cause of COPD: Tobacco smoke
Research shows that tobacco smoke stands as the single biggest cause of COPD worldwide.
- In high-income countries, tobacco accounts for the majority of COPD cases.
- Cigarette smoke irritates and inflames the airways thousands of times over many years.
- The immune system responds with chronic inflammation that eventually remodels the airway walls and destroys alveoli.
Important nuance:
Not every smoker develops COPD, but every smoker raises risk in a predictable dose–response pattern. Heavy, long-term smoking delivers the highest risk.
If you smoke and ask, “Will I develop COPD?”, statistics do not give comfort. Long-term smokers carry multiple-fold higher risk of chronic obstructive pulmonary disease compared with never-smokers.
5.2 Air pollution and indoor smoke
In many countries, especially where households cook with biomass fuels (wood, dung, charcoal) in poorly ventilated spaces, indoor air pollution becomes the main cause of COPD for non-smoking women.
Other contributors:
- Urban air pollution from traffic and industry
- Second-hand smoke in homes, bars, and workplaces
Chronic inhalation of these pollutants injures airway lining cells and amplifies inflammation.
5.3 Occupational exposures
Certain jobs dramatically raise COPD risk:
- Coal miners, construction workers, and quarry workers breathe dust daily.
- Factory workers inhale various fumes and chemicals.
- Farmers inhale organic dust and ammonia in poorly ventilated barns.
According to occupational lung disease studies, long-term exposure in these settings explains a significant fraction of COPD in people who never touch cigarettes.
5.4 Genetics and lung development
A smaller, but crucial group:
- People born with alpha‑1 antitrypsin deficiency, a genetic condition.
- This protein normally protects lung tissue.
- Without enough of it, the lung breaks down under even modest smoke or pollution exposure.
- People who experienced poor lung growth in childhood:
- Premature birth, severe early-life infections, malnutrition, or heavy passive smoke exposure reduce peak lung function in early adulthood.
These individuals enter adult life with lower “lung reserve,” so they reach symptomatic COPD earlier.
5.5 The real message about the cause of COPD
The common cause most people recognize: cigarette smoking.
The wider truth every reader should carry:
COPD develops when the lungs face harmful particles or gases for years, especially tobacco smoke, biomass fuel smoke, workplace dusts, and urban pollution. Genetics and early-life lung health influence who gets sick first.
If you remove the exposure early enough, you radically change the story.
6. COPD in the Medical Context: How Clinicians Think About It
In clinics, doctors do not just see “a smoker with a cough.” They think in patterns:
- Chronic symptoms: How long has the cough and breathlessness persisted?
- Risk factors: Smoking history, workplace exposure, home cooking fuels, city air, childhood infections.
- Objective airflow limitation: Spirometry measurements.
- Exacerbations: How many flare-ups and hospital visits each year?
- Impact on daily life: Stairs, shopping, self-care, work.
This perspective matters because early diagnosis changes the trajectory. Research shows that people diagnosed and treated in mild to moderate stages maintain better lung function and quality of life for longer.
So if you fit any risk pattern above and notice respiratory symptoms, you already have a clear signal: schedule a lung check rather than waiting for “serious trouble.”
7. What Is COPD in Medical Terms? Symptoms and Progression
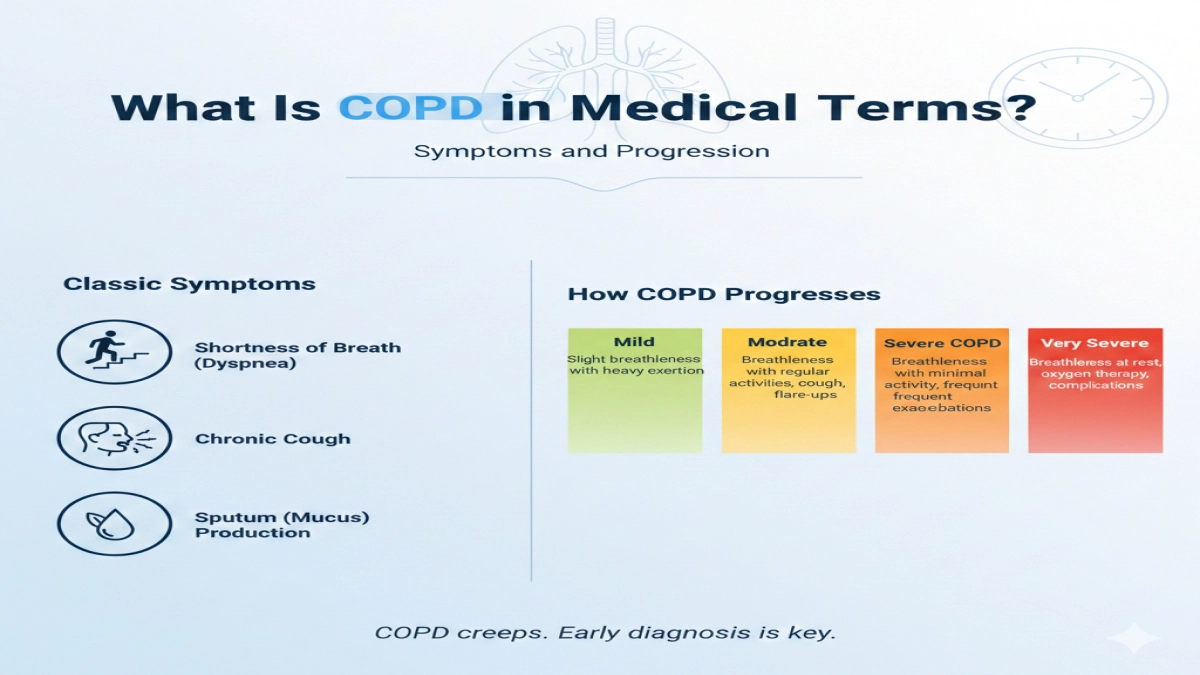
People with COPD rarely wake up one day unable to breathe. COPD creeps.
7.1 Classic symptoms of COPD
Doctors describe a triad of key features:
- Shortness of breath (dyspnea)
- Starts with exertion: climbing hills, rushing to catch a bus.
- Progresses to daily activities: dressing, showering, carrying groceries.
- In severe COPD, even talking or eating triggers breathlessness.
- Chronic cough
- Lasts at least three months in a year for two consecutive years in classic chronic bronchitis.
- May sound dry at first, then “chesty.”
- Sputum (mucus) production
- White, yellow, or greenish secretions.
- Patients describe “bringing up phlegm every morning” or “clearing my throat all day.”
Other common complaints:
- Wheeze or noisy breathing
- Chest tightness
- Fatigue and reduced exercise tolerance
- Frequent “chest infections” or “bronchitis” episodes
When we talk about symptoms of COPD, these signs sit at the core.
7.2 How COPD progresses
Think of COPD progression in four broad stages (GOLD groups airflow limitation by FEV₁, a spirometry measure):
- Mild COPD
- Slight breathlessness with heavy exertion
- Chronic cough ignored or blamed on smoking
- Lung tests show reduced airflow, but daily life still feels manageable.
- Moderate COPD
- Breathlessness with regular activities (hills, stairs)
- Cough and sputum more persistent
- First flare-ups that need steroids, antibiotics, or urgent visits.
- Severe COPD
- Breathlessness with minimal activity: walking across the room, getting dressed
- Frequent exacerbations (two or more flare-ups a year, or at least one hospitalization)
- Significant weight loss, muscle weakness, and social withdrawal.
- Very severe COPD
- Breathlessness at rest
- Oxygen therapy, repeated hospital stays
- Complications such as pulmonary hypertension (high blood pressure in lung arteries), right-sided heart strain, and respiratory failure.
Specialists interpret lung function, symptoms, and exacerbation history together to stage severity and guide treatment.
7.3 A typical case: how people ignore early signs
Imagine this real-world pattern, which appears again and again in clinics:
- A 55‑year‑old construction worker smokes a pack a day.
- He wakes with a cough and spits out mucus every morning.
- Climbing two flights of stairs leaves him winded, but he shrugs it off as “getting older.”
- He catches “bronchitis” several winters in a row. Each time, he receives antibiotics without lung tests.
- Ten years later, a doctor finally runs spirometry. The test shows clear, fixed airflow limitation: moderate to severe COPD.
That entire decade represented a missed window for earlier diagnosis, counseling, and pulmonary rehabilitation that would have preserved more lung function.
8. COPD According to GOLD: The Global Reference Standard
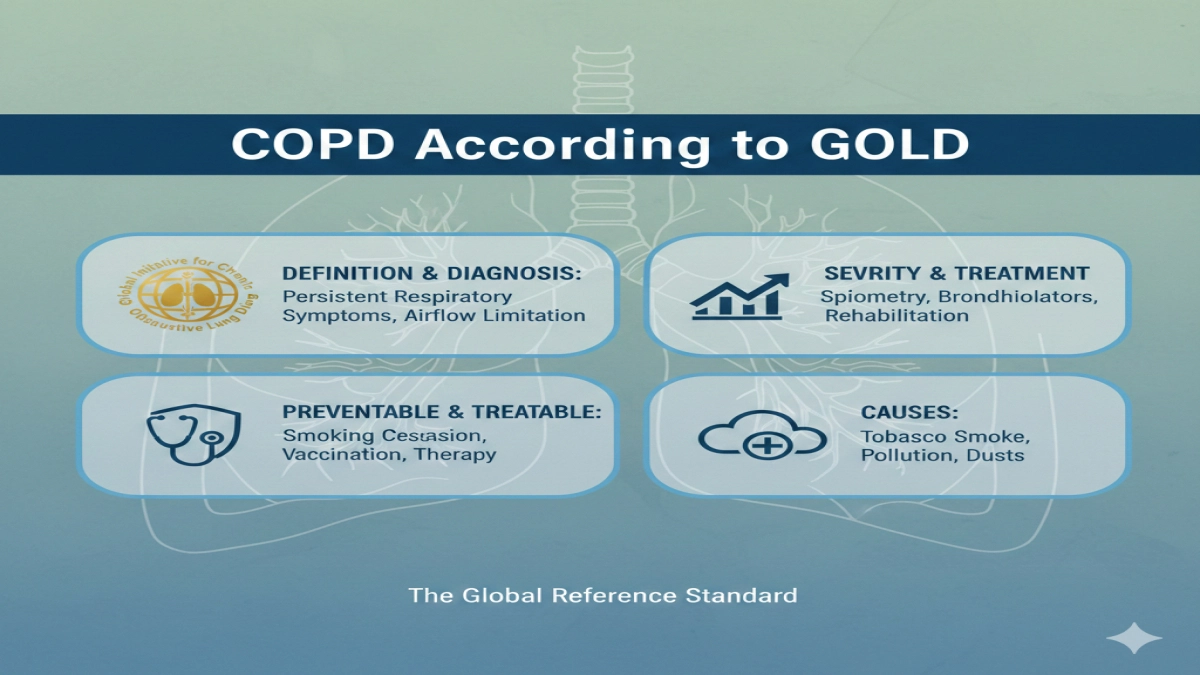
When clinicians want a precise, shared language for COPD, they turn to GOLD — the Global Initiative for Chronic Obstructive Lung Disease.
The name itself covers two of your NLP phrases:
- “global initiative for chronic obstructive”
- “initiative for chronic obstructive lung”
GOLD gathers experts worldwide to produce a regularly updated strategy document on:
- COPD definition and diagnosis
- Severity assessment
- Treatment pathways
- Prevention strategies
8.1 The GOLD definition (latest available evidence)
As of my latest evidence (up to October 2024), GOLD defined COPD as:
A common, preventable, and treatable disease characterized by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities, usually caused by significant exposure to noxious particles or gases.
Key components:
- Common – COPD affects hundreds of millions of people globally.
- Preventable and treatable – Smoking cessation, vaccination, inhaler therapy, and pulmonary rehabilitation change outcomes at every stage.
- Persistent symptoms – Cough, mucus, and breathlessness never fully clear.
- Airflow limitation – Spirometry confirms reduced FEV₁/FVC ratio that does not fully normalize after bronchodilator medication.
- Airway and alveolar abnormalities –
- Airway inflammation and remodeling (chronic bronchitis).
- Alveolar destruction and loss of elastic recoil (emphysema).
- Exposure to noxious particles or gases – Tobacco smoke, occupational dusts and chemicals, air pollution, indoor biomass smoke.
GOLD serves as the reference for research studies, guidelines, and national policies.
9. Understanding the GOLD 2025 COPD Definition
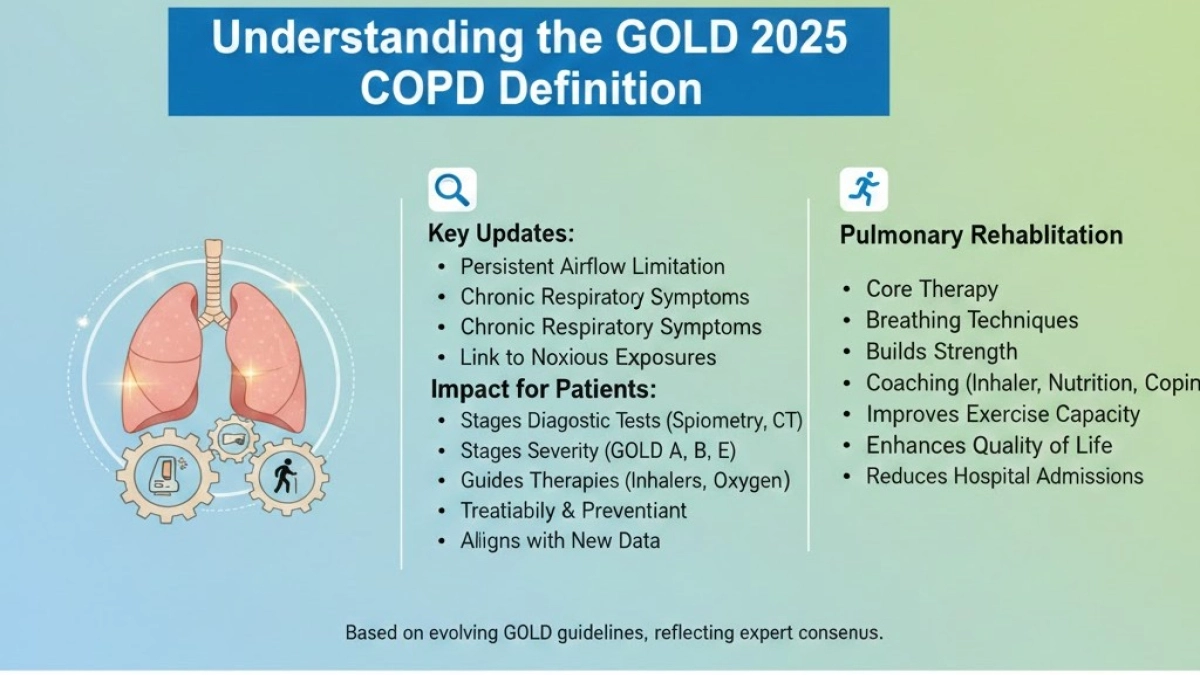
The GOLD 2025 update builds on previous definitions rather than replacing them with something entirely new. While I do not access documents published after October 2024, recent GOLD revisions follow a clear pattern:
- They sharpen the language around:
- Persistent airflow limitation
- Chronic respiratory symptoms
- The link to noxious exposures
- They emphasize treatability and prevention even in advanced disease.
- They align the definition with new data on risk factors, comorbidities, and imaging findings.
9.1 Why the GOLD framework matters for patients
For people with COPD and their families, GOLD does more than set academic definitions.
It shapes:
- Which tests your doctor orders – particularly spirometry and, where needed, CT scans.
- How your doctor stages severity – combining airflow limitation, symptoms, and exacerbation risk into GOLD A, B, E groups.
- Which inhalers or therapies you receive – bronchodilators, dual or triple therapy, and when to add oxygen or refer for lung volume reduction or transplant.
For example:
- A patient with moderate airflow limitation but frequent severe flare-ups lands in a higher-risk GOLD group.
- That patient receives more aggressive inhaler therapy and closer follow-up, not just “keep doing what you’re doing.”
9.2 GOLD and pulmonary rehabilitation
GOLD treats pulmonary rehabilitation as a core therapy rather than a “nice bonus.”
Pulmonary rehabilitation programs:
- Teach breathing techniques that reduce breathlessness.
- Build leg and core strength so daily activities feel easier.
- Coach patients on inhaler technique, nutrition, and coping skills.
A Cochrane review of pulmonary rehabilitation showed:
- Clear improvement in exercise capacity.
- Better quality of life.
- Fewer hospital admissions.
GOLD 2025 continues this emphasis: rehabilitation stands beside pharmacologic treatment, not behind it.
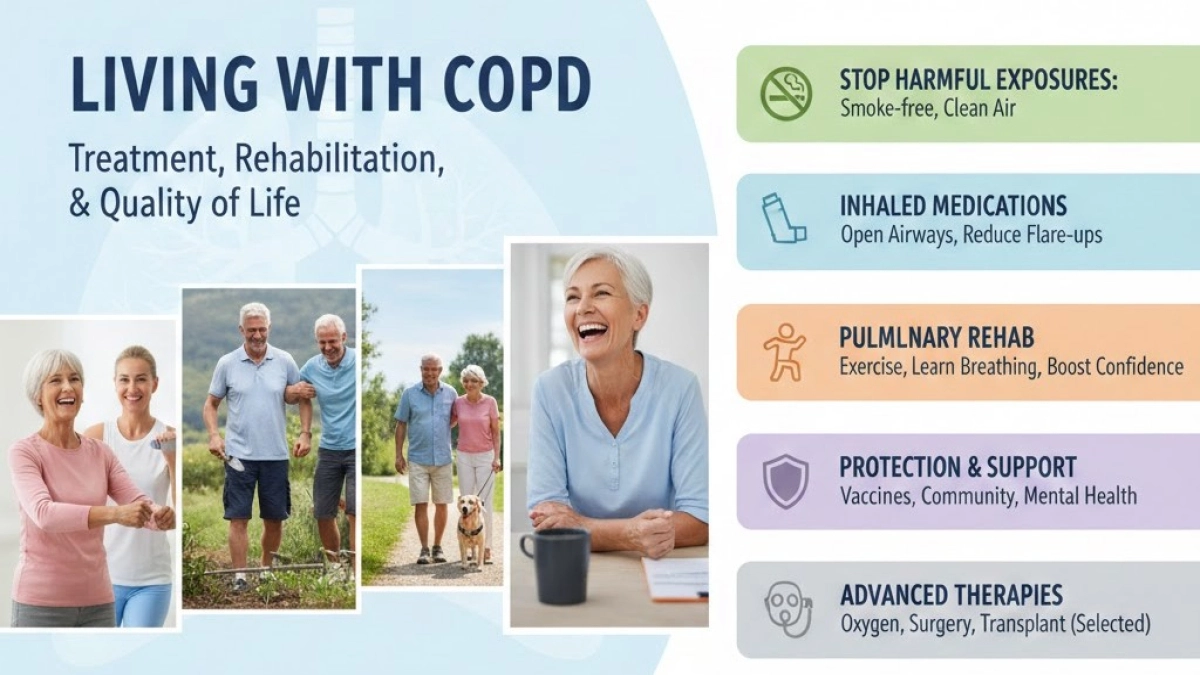
10. Living With COPD: Treatment, Rehabilitation, and Quality of Life
Once you understand the disease, the next question appears fast: “What can I do about it?”
10.1 Core treatment pillars
Doctors build COPD management around several pillars:
- Stop harmful exposures
- Smoking cessation programs, nicotine replacement, prescription medicines.
- Workplace protections and masks where dust or fumes persist.
- Cleaner cooking fuels and better household ventilation.
- Inhaled medications
- Bronchodilators open airways (short- and long-acting).
- Inhaled corticosteroids for people with frequent exacerbations or overlap with asthma.
- Combination inhalers tailored to GOLD group and exacerbation history.
- Pulmonary rehabilitation
- Supervised exercise training
- Education and breathing techniques
- Psychological and social support
Research shows that patients who complete rehab programs walk farther, feel less breathless, and rate their quality of life higher.
- Vaccinations and infection control
- Influenza, pneumococcal, and COVID‑19 vaccines reduce severe infections and hospitalizations.
- Oxygen and advanced therapies
- Long-term oxygen therapy for patients with severely low oxygen levels.
- Surgical or bronchoscopic lung volume reduction in selected emphysema cases.
- Lung transplant for a small, carefully chosen group with very severe COPD.
10.2 How pulmonary rehabilitation changes daily life
Many people with COPD picture rehab as “just a gym program.” It reaches far beyond that.
A typical program:
- Starts with a gentle 6‑minute walk test to assess baseline.
- Builds a tailored routine: treadmill or corridor walking, cycling, light resistance training.
- Teaches pursed-lip breathing and diaphragmatic breathing to control breathlessness.
- Includes group sessions on nutrition, energy conservation, and coping with anxiety.
Here’s a composite real-world scenario based on patient reports from rehab programs:
A 62‑year‑old ex-smoker with moderate COPD arrives for the first rehab session. Walking from the parking lot already leaves him short of breath. Over eight weeks, he attends sessions twice a week. By the end, he walks 400 meters in the 6‑minute test instead of 220. He dresses without pausing to catch his breath and returns to light gardening, which he had abandoned years ago.
No miracle cure took place. He learned to use his remaining lung function more effectively, strengthened his muscles, and gained confidence. Pulmonary rehabilitation delivers that combination.
10.3 Quality of life with COPD: more than lung numbers
Spirometry results matter, but they do not tell the full story.
People with COPD describe:
- Fear of leaving home in case breathlessness strikes.
- Embarrassment over cough or sputum in public.
- Guilt about smoking history even when they now stay smoke‑free.
- Lost roles: grandparent who cannot play on the floor, worker who retired early.
A strong COPD care plan addresses:
- Physical capacity – through rehab, nutrition, and appropriate inhalers.
- Psychological health – screening for anxiety and depression; counseling when needed.
- Social connection – support groups, community programs, online forums.
You deserve a plan that treats you as more than a lung function number.
11. Complications of Severe COPD: Why Early Action Pays Off
As COPD progresses without adequate treatment, complications build up.
11.1 Pulmonary hypertension and heart strain
When COPD destroys alveoli and narrows small vessels, the pressure in lung arteries rises. This state, known as pulmonary hypertension, forces the right side of the heart to pump harder.
Consequences:
- Swollen ankles
- Liver congestion and abdominal discomfort
- Worsening fatigue and breathlessness
Cardiologists call this cor pulmonale when COPD drives the problem. Early control of COPD and oxygen therapy when indicated reduce this risk.
11.2 Exacerbations: acute flare-ups
Exacerbations define much of the suffering and cost in COPD care. They involve:
- Sudden spike in breathlessness
- Increased cough and sputum volume or change in color
- Need for steroids, antibiotics, or emergency care
Research shows that:
- Each severe exacerbation accelerates lung function decline.
- Recent exacerbations predict further flare-ups.
This creates a vicious cycle in severe COPD. Breaking the cycle with optimal inhaler therapy, vaccines, rehab, and smoking cessation becomes a top priority.
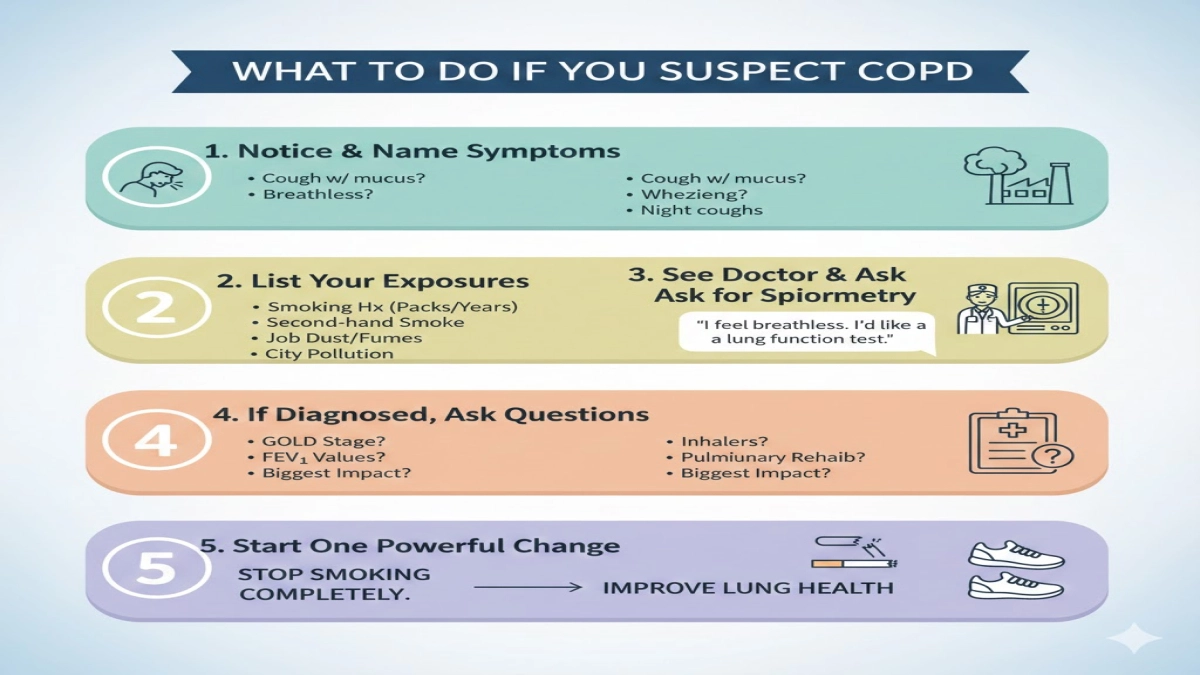
12. What To Do If You Suspect COPD: A Step-by-Step Guide
You came here with a question. This is where that curiosity turns into action.
Step 1: Notice and name your symptoms
Ask yourself:
- Do I cough with mucus most days for months?
- Do I feel more breathless than friends my age when walking or climbing stairs?
- Do I wheeze or hear noisy breathing?
- Do I wake at night short of breath or with coughing fits?
If you answer “yes” to several questions and live with any smoking or pollution exposure history, you carry a real signal, not “just getting older.”
Step 2: List your exposures
Write down:
- Cigarette, cigar, or pipe smoking history (packs per day × years)
- Second-hand smoke in home or work
- Job roles involving dust, fumes, or chemicals
- Home cooking fuels and ventilation
- Major city pollution exposure
Doctors spot patterns faster when you present this clearly.
Step 3: See your primary doctor and ask for spirometry
Spirometry remains the cornerstone of COPD diagnosis.
Practical tip: use a direct request such as:
“I feel breathless with ordinary activity, and I’ve smoked for years. I’d like a formal lung function test, including spirometry, to check for COPD or other lung disease.”
This keeps the conversation focused. Bring your symptom and exposure notes.
Step 4: If COPD diagnosis appears, ask the right questions
Key questions to ask:
- Which GOLD stage or group do I fall into?
- What are my FEV₁ and FEV₁/FVC values?
- Which inhalers will I start, and how do I use them correctly?
- Can you refer me to a pulmonary rehabilitation program?
- What steps give me the biggest impact this year?
You move from passive recipient to active partner when you ask these questions.
Step 5: Start one powerful change immediately
For most people with COPD, the single highest-impact change remains clear:
Stop smoking completely and permanently.
Experts describe smoking cessation as the most effective intervention across all COPD stages. It slows lung function decline, reduces exacerbations, and improves survival.
If you already quit, celebrate that win and focus on rehab, inhaler technique, and activity.
13. Recap: What COPD Really Is — and Why That Definition Matters
If you remember one sentence, let it be this:
COPD means long-term damage to the lungs that narrows airways and blocks airflow, causing breathlessness and chronic cough — but with treatment, you still gain control and protect quality of life.
You now understand:
- What COPD stands for and what chronic obstructive lung disease includes.
- How emphysema and chronic bronchitis combine inside the lung.
- The main cause of COPD and other risk factors beyond smoking.
- How medical teams define, diagnose, and stage COPD using GOLD criteria.
- Why pulmonary rehabilitation, inhalers, and lifestyle change reshape daily life.
- How severe COPD leads to complications such as pulmonary hypertension, and why early action prevents or delays them.
You also hold a practical path: notice symptoms, track exposures, ask for spirometry, and push for rehab and comprehensive care.
Health search sessions end when the reader feels, “I understand what this is, and I know my next move.”
If this article brought you to that point, your time here paid off.
People Also Ask: Short, Direct Answers
1. Is COPD the same thing as asthma?
No. Both cause airflow obstruction and breathlessness, but asthma typically starts earlier in life, responds strongly to inhaled steroids, and shows more reversible airflow limitation on spirometry. COPD usually appears later, especially after years of exposure to smoke or pollution, and the airflow limitation stays largely fixed. Some people have features of both conditions, which doctors call asthma–COPD overlap.
2. Can a non-smoker develop COPD?
Yes. Significant exposure to biomass fuel smoke, workplace dusts and fumes, severe early-life lung infections, and genetic factors such as alpha‑1 antitrypsin deficiency all lead to COPD in non-smokers. In some regions, especially rural areas that rely on indoor biomass cooking, non-smoking women carry very high COPD risk.
3. Can COPD get better with treatment?
Damaged lung tissue does not regenerate, so the structural changes stay. However, treatment reduces inflammation, opens airways, rebuilds muscle strength, and stabilizes lung function. Many people with COPD walk farther, climb more stairs, and report better quality of life after they start a comprehensive management plan.
4. How long can you live with COPD?
Life expectancy depends on many factors: stage at diagnosis, smoking status, exacerbation frequency, other diseases (such as heart disease or diabetes), and adherence to treatment. Research shows that people who quit smoking, stay active, attend pulmonary rehabilitation, and follow guideline-based care live significantly longer than similar patients who do not.[^6] Your own doctor can estimate risk more precisely once they review your tests.
5. Does COPD always lead to oxygen therapy?
No. Many people with mild or moderate COPD never need oxygen. Long-term oxygen therapy enters the picture when blood oxygen levels fall below specific thresholds at rest or during exertion. Physicians measure this with arterial blood gases and pulse oximetry. Early treatment, smoking cessation, and rehab reduce the chance of reaching that point.
6. Why do some reports say “COPD may cause heart problems”?
Medical reports sometimes use phrases like “COPD may increase the risk of pulmonary hypertension and right heart failure” to reflect statistical risk, not certainty. Large studies show a strong association between chronic obstructive pulmonary disease and cardiovascular disease, so cardiology and respiratory teams monitor heart health closely in people with COPD.
References
-
Global Initiative for Chronic Obstructive Lung Disease (GOLD).
Global Strategy for the Diagnosis, Management, and Prevention of COPD.
GOLD Reports 2024–2025 Update. -
World Health Organization (WHO).
Chronic Obstructive Pulmonary Disease (COPD): Key Facts.
WHO, Geneva. -
Centers for Disease Control and Prevention (CDC).
COPD: Causes, Risk Factors, and Symptoms.
National Center for Chronic Disease Prevention and Health Promotion. -
Salvi S, Barnes PJ.
Chronic obstructive pulmonary disease in non-smokers.
Medical Disclaimer
Information on this website is for general education only. It is not medical advice.
The content on COPD.MEDLIFEGUIDE is written to help people understand COPD and other breathing conditions in a clear and simple way. It is not a substitute for professional medical care, diagnosis, or treatment.
Always talk to a licensed healthcare provider for personal medical concerns.
Do not ignore symptoms or delay getting help because of something you read on this site. If you think you may be having a medical emergency, call your local emergency number right away.
Leave a Reply