
Quick Summary
The GOLD criteria for COPD provide a standardized method to diagnose, classify, and manage chronic obstructive pulmonary disease using spirometry results, symptom burden, and exacerbation history. Accurate staging guides treatment decisions and improves patient outcomes.
What Is COPD?
Chronic obstructive pulmonary disease (COPD) is a long-term lung condition that blocks airflow and makes breathing difficult. It includes:
- Chronic bronchitis (long-term cough with mucus)
- Emphysema (damage to air sacs in the lungs)
COPD is progressive, meaning it worsens over time if untreated.
What Are the GOLD Criteria for COPD?
The GOLD criteria are guidelines developed by the Global Initiative for Chronic Obstructive Lung Disease. These criteria are used worldwide to:
- Confirm COPD diagnosis
- Measure severity
- Guide treatment plans
The GOLD system relies on three main components:
- Spirometry (lung function testing)
- Symptom assessment
- Exacerbation history
GOLD Criteria for COPD Diagnosis
Spirometry Requirement
COPD diagnosis requires spirometry confirmation.
Key diagnostic threshold:
- Post-bronchodilator FEV1/FVC ratio < 0.70
Definitions:
- FEV1: Forced expiratory volume in 1 second
- FVC: Forced vital capacity
If the ratio is below 0.70 after using a bronchodilator, airflow limitation is considered persistent and consistent with COPD.
GOLD Staging Based on Airflow Limitation
Once COPD is confirmed, severity is graded using FEV1 percentage.
| GOLD Stage | Severity Level | FEV1 (% predicted) |
|---|---|---|
| GOLD 1 | Mild | ≥ 80% |
| GOLD 2 | Moderate | 50–79% |
| GOLD 3 | Severe | 30–49% |
| GOLD 4 | Very Severe | < 30% |
This staging reflects lung function impairment only.
Symptom Assessment Tools
mMRC Dyspnea Scale
Measures breathlessness:
- Grade 0: Breathless only with heavy exercise
- Grade 1: Shortness of breath when walking fast
- Grade 2: Walks slower than peers due to breathlessness
- Grade 3: Stops after walking 100 meters
- Grade 4: Too breathless to leave home
COPD Assessment Test (CAT)
An 8-question tool scoring symptoms from 0 to 40.
- Low impact: CAT < 10
- High impact: CAT ≥ 10
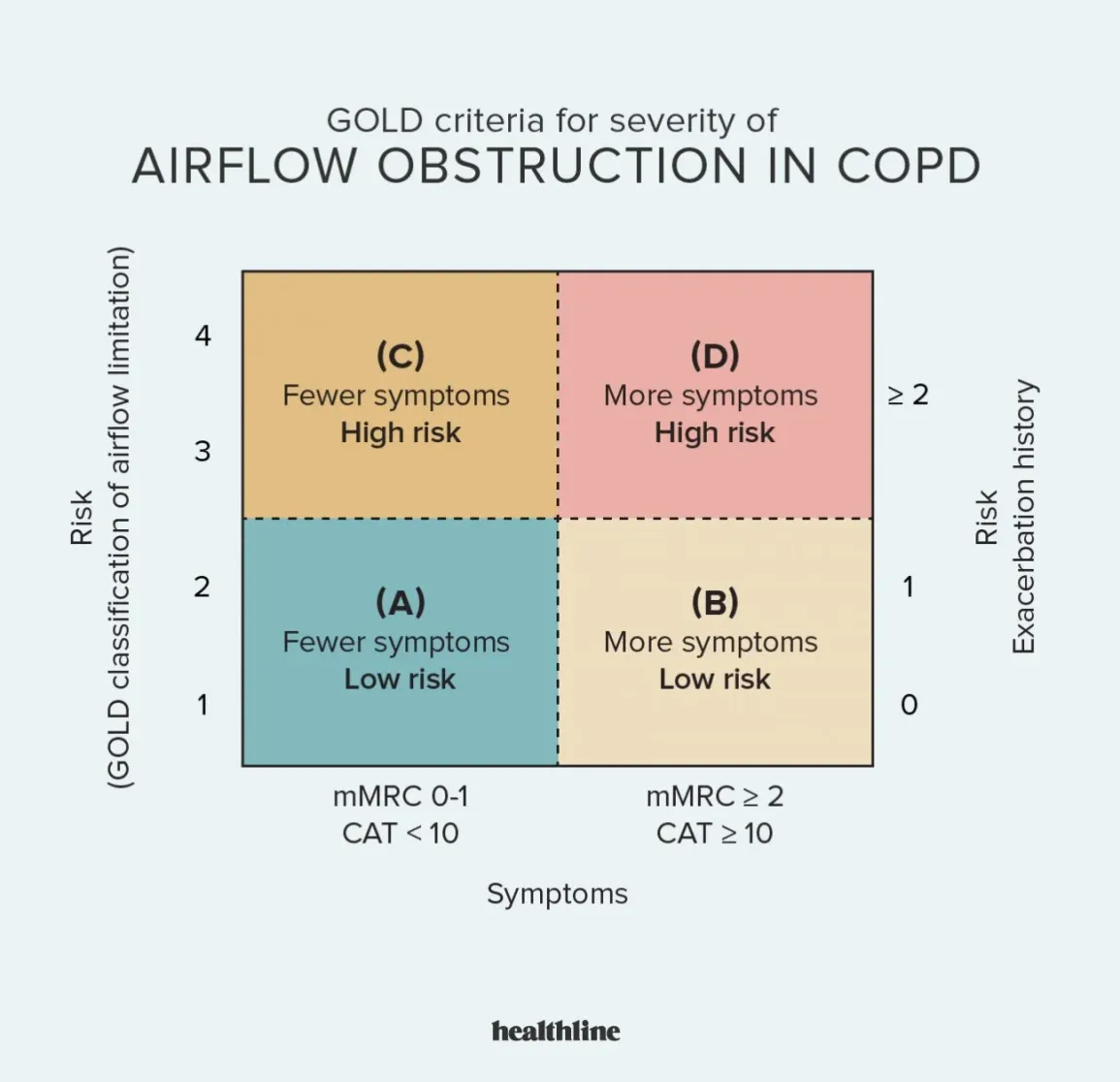
GOLD ABCD Grouping System
Patients are classified into groups A, B, E (updated GOLD model) based on:
- Symptoms (CAT or mMRC)
- Exacerbation history
| Group | Symptoms | Exacerbations |
|---|---|---|
| A | Low | 0–1 (no hospitalization) |
| B | High | 0–1 (no hospitalization) |
| E | Any | ≥2 OR ≥1 hospitalization |
This system replaces older ABCD models and focuses more on exacerbation risk.
Treatment Based on GOLD Criteria
Group A
- Bronchodilator (short or long-acting)
Group B
- Long-acting bronchodilator (LABA or LAMA)
Group E
- Combination therapy (LABA + LAMA)
- Consider inhaled corticosteroids if eosinophils are elevated
Role of Exacerbations in COPD
Exacerbations are sudden worsening episodes that require medical care.
Risk factors include:
- Prior exacerbations
- Smoking
- Infections
- Poor medication adherence
Frequent exacerbations accelerate lung function decline.
Risk Factors for COPD
- Cigarette smoking (primary cause)
- Air pollution exposure
- Occupational dust and chemicals
- Genetic factors (e.g., alpha-1 antitrypsin deficiency)
Unique Clinical Takeaways
1. Spirometry Alone Is Insufficient for Full Disease Burden Assessment
While the FEV1/FVC ratio confirms COPD, symptom severity often does not correlate directly with airflow limitation. Patients with moderate airflow restriction may experience severe symptoms due to hyperinflation or muscle deconditioning. Clinical management must integrate CAT or mMRC scores to avoid under-treatment.
2. Exacerbation History Predicts Future Risk More Than FEV1
Data from longitudinal studies show that previous exacerbations are the strongest predictor of future episodes. A patient with relatively preserved lung function but frequent exacerbations may require more aggressive therapy than a patient with severe airflow limitation but stable symptoms.
3. Blood Eosinophil Count Guides Steroid Use
Recent GOLD updates emphasize blood eosinophil levels as a biomarker. Patients with eosinophil counts ≥300 cells/µL benefit more from inhaled corticosteroids. Low eosinophil levels (<100 cells/µL) are associated with reduced steroid response and increased pneumonia risk.
4. Misdiagnosis with Asthma Remains Common
COPD and asthma overlap in symptoms such as wheezing and airflow limitation. However:
- Asthma shows reversible airflow obstruction
- COPD shows persistent limitation
Failure to distinguish leads to inappropriate therapy, especially overuse of steroids.
5. Early COPD Often Goes Undetected
Patients may have significant lung damage before symptoms become noticeable. Routine spirometry in high-risk individuals (e.g., long-term smokers) improves early detection and slows disease progression with timely intervention.
Monitoring and Follow-Up
Patients require ongoing evaluation:
- Spirometry annually
- Symptom reassessment (CAT or mMRC)
- Exacerbation tracking
- Medication review
Prevention Strategies
- Smoking cessation (most effective intervention)
- Vaccination (influenza and pneumococcal)
- Air quality improvement
- Pulmonary rehabilitation
Prognosis of COPD Based on GOLD Criteria
Prognosis depends on:
- GOLD stage
- Frequency of exacerbations
- Comorbid conditions
- Smoking status