
Chronic obstructive pulmonary disease (COPD) is a long-term lung disease that makes it hard to breathe. The most common symptoms of COPD include a chronic cough, daily mucus, shortness of breath with routine activities, wheezing, and repeated “chest infections.” In early stages, many people with COPD think they are just “out of shape” or “getting older,” which delays diagnosis.
If you notice a persistent cough, breathlessness when walking on flat ground, or frequent bronchitis, COPD should be considered and you need a pulmonary function test. Sudden worsening breathlessness, blue lips or fingers, or confusion signal a COPD exacerbation and require urgent or emergency care.
Quick Summary
Key Points
- COPD means chronic obstructive pulmonary disease – mostly chronic bronchitis and emphysema – a chronic lung disease that blocks airflow and damages the lung.
- The main cause of COPD worldwide is long-term smoking; exposure to dust, fumes, biomass fuel, and air pollution also increases the risk of COPD.
- Early COPD symptoms: chronic cough, daily phlegm, and getting short of breath on stairs or hills long before others your age.
- Common symptoms of COPD include: breathlessness, wheeze, chest tightness, recurrent “bronchitis,” fatigue, and reduced exercise tolerance.
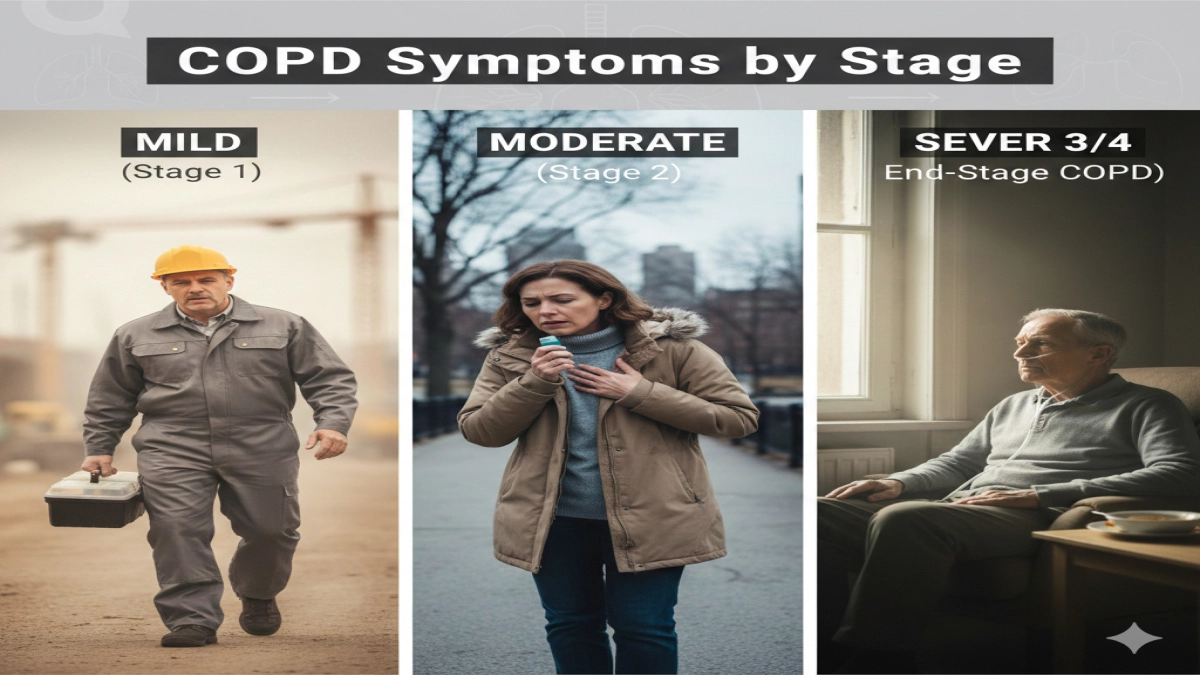
- Symptoms by stage:
- Stage 1: mild breathlessness with heavy exertion, “smoker’s cough.”
- Stage 2: shortness of breath with normal walking; more flare-ups.
- Stage 3: breathless with simple tasks like dressing; big impact on quality of life.
- End-stage or severe COPD: breathless at rest, weight loss, frequent acute exacerbations of COPD, possible pulmonary hypertension and heart strain.
- Red flags of COPD that need urgent care: sudden breathing worse than usual, chest pain, confusion, blue lips/fingers, fast heartbeat, or no relief from usual inhalers.
- Diagnosis of COPD requires a pulmonary function test (spirometry) – no test, no reliable diagnosis.
- Treating COPD: inhalers, vaccines, oxygen when needed, and especially a pulmonary rehabilitation program improve symptoms and quality of life and reduce mortality in COPD.
- COPD is permanent and progressive, but COPD is largely preventable and COPD treatments can slow progression and improve daily life.
If you think “this sounds like me,” your next step is simple: ask your primary care professional for spirometry to diagnose COPD or rule it out.
1. Introduction:
Here is the part that surprises many people:
According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD), COPD is already one of the top three causes of death worldwide, yet up to half of cases of COPD stay undiagnosed until the disease sits in a moderate or severe stage.
Many people living with COPD blame their chronic cough, breathlessness, and fatigue on aging, weight, or being “out of shape.” By the time they hear the phrase chronic obstructive pulmonary disease for the first time, their lungs already lost a lot of reserve.
You landed on this page for a reason. You might:
- Have a cough that refuses to go away
- Get winded walking across a parking lot
- Wonder if your “bronchitis every winter” relates to COPD
- Care for a patient with COPD and want clear explanations
This guide gives you:
- A plain-language explanation of symptoms of COPD by stage
- The difference between mild, moderate, and severe COPD
- The red flags that demand urgent medical help
- How doctors diagnose COPD with pulmonary function testing
- Concrete steps to protect your lung health and prevent COPD from getting worse
If you read through with your own symptoms in mind, you will finish with a realistic picture of where you stand and what to do next.
2. Understanding COPD
2.1 What is COPD?
COPD stands for chronic obstructive pulmonary disease. It describes a group of chronic lung conditions that block airflow and make exhalation difficult. The common types of COPD include:
- Emphysema – damage and destruction of air sacs in the lung
- Chronic bronchitis – long-term inflammation and narrowing of the airways
In clinical practice, many doctors talk about “emphysema and chronic bronchitis” as the main components of COPD. GOLD, the global initiative for chronic obstructive lung disease, defines COPD as a chronic respiratory disease with persistent airflow limitation and chronic respiratory symptoms.
COPD is a lung disease, but it does not stay “just a lung problem” for long. As COPD progresses, it affects the heart, muscles, metabolism, and emotional health, and it significantly reduces quality of life.
2.2 Common causes and risk factors
Research shows that one common cause dominates:
- Cigarette smoking – The biggest risk factor for COPD by far
Major studies show smoking explains up to 75% of COPD cases in many countries. In that sense, COPD is largely preventable.
Important risk factors for COPD and common causes of COPD include:
- Long-term cigarette smoking and second-hand smoke
- Household biomass smoke exposure (wood, charcoal, dung for cooking/heating)
- Workplace dusts and fumes (mining, construction, factories, agriculture)
- Urban air pollution
- Severe childhood lung infections that damage growing lungs
- Genetic conditions such as alpha-1 antitrypsin deficiency
So the cause of COPD is rarely “bad luck.” Lung specialists see a pattern: long-term exposure to harmful particles injures the airways, drives inflammation in COPD, and sets up chronic obstructive lung disease.
2.3 Impact of COPD on daily life
For a patient with COPD, this is not abstract pathology. It shows up as:
- Struggling to climb one flight of stairs
- Planning the day around when you can rest
- Turning down invitations because “the walk from the parking lot is too far”
- Bringing rescue inhalers everywhere “just in case”
A typical scenario:
“Imagine a delivery driver in his mid‑50s. Ten years ago he smoked a pack a day and brushed off a nagging cough. Now he stops mid‑route to catch his breath, leans on the truck, and tells himself he needs to ‘get back in shape.’ That pattern matches the early development of COPD, not just aging.”
COPD affects work, family roles, intimacy, and independence. That is why understanding symptoms early changes the burden of COPD on your life later.
3. What Are the Symptoms of COPD?
3.1 General symptoms experienced by people with COPD
Across countries and cultures, COPD patients describe the same cluster of problems:
- Chronic cough – present for months or years
- Daily sputum (phlegm) – white, yellow, or clear
- Breathlessness (dyspnea) – especially with exertion
- Wheezing – whistling when breathing out
- Chest tightness or heaviness
- Recurrent “chest infections” – bronchitis or pneumonia
- Fatigue and low stamina
These common symptoms of COPD build slowly. That slow change tricks people with COPD into normalizing them: “I always cough like this,” or “I just have bad lungs every winter.”
3.2 Why symptom awareness matters
Here is the hard truth: COPD is a progressive disease. COPD is a long-term, chronic lung disease and COPD is permanent – once the airways and air sacs scar and collapse, you cannot fully reverse that damage with any current cure for COPD.
However, when you catch COPD symptoms early and tackle the management of COPD aggressively:
- You slow the rate of COPD decline in lung function
- You cut acute exacerbations of COPD, hospitalizations, and mortality in COPD
- You protect your quality of life and independence
That is why noticing subtle changes in your breathing now matters far more than waiting for severe COPD symptoms later.
4. Signs and Symptoms of COPD
4.1 Detailed list of common signs
Symptoms of COPD (what you feel and describe):
- Persistent, “nagging” chronic cough
- Coughing up mucus most days for three months or longer in a year
- Shortness of breath walking on flat ground or climbing a single flight of stairs
- Needing to stop to catch your breath when others keep walking
- Wheezing or noisy breathing, especially when exhaling
- Chest tightness, heaviness, or “air hunger”
- Waking at night feeling breathless
- Unintentional weight loss in advanced disease
- Fatigue that makes ordinary tasks feel huge
Signs of COPD (what others can see or what clinicians detect):
- Barrel-shaped chest (from overinflated lungs)
- Use of neck or shoulder muscles to breathe
- Pursed-lip breathing
- Reduced breath sounds and prolonged exhalation on exam
- Swollen ankles (possible right-heart strain or pulmonary hypertension)
- Cyanosis (blue lips or fingertips) in advanced or acute COPD
- Lower oxygen levels on pulse oximeter
- Abnormal pulmonary function results on spirometry
4.2 Signs vs symptoms in real life
Here’s why this distinction matters. A person can have “quiet” signs of COPD on a pulmonary function test years before symptoms scare them. At the same time, a person can feel very breathless with relatively mild numeric changes, especially during an acute COPD flare.
If your story includes long-term smoking plus a chronic cough with sputum, COPD should be considered, even if you still “push through” daily life.
5. Early COPD Symptoms
5.1 How early COPD feels
In stage 1, people with COPD often just feel “slower” than they used to. Typical early features of COPD:
- Cough in the morning that “warms up” the lungs
- Needing extra time on hills or stairs
- Chest tightness when you hurry to catch a bus
- More “bronchitis” episodes than friends or family
- “I can’t keep up with my grandchildren like I should”
Many people with COPD often blame allergies, weight gain, or lack of exercise. That delay gives the development of COPD time to accelerate under the surface.
5.2 Why early detection matters
Research from large cohorts and the epidemiology of COPD literature shows:
- People who receive treatment and participate in a pulmonary rehabilitation program in the earlier stages preserve more lung function.
- They also show fewer flare-ups, less COPD exacerbation, better exercise tolerance, and improved mood.
Early detection lets you:
- Quit smoking while you still have meaningful pulmonary function reserve
- Start inhaled therapies that reduce inflammation in COPD
- Learn breathing techniques and exercise strategies that reshape your daily routine
From a practical standpoint, the best way to prevent COPD from getting worse is to catch it during this early window.
5.3 What does Stage 1 COPD feel like?
People describe Stage 1 COPD like this:
- “I can do everything; I just get winded faster.”
- “If I climb three flights of stairs, I’m breathing harder than my friends.”
- “I cough most mornings; it clears up, so I ignore it.”
On testing, a pulmonary function test already shows airflow obstruction. The person, however, still lives what feels like a relatively stable COPD life.
A GOLD-based view:
- FEV1 (a key spirometry number) stays above 80% predicted
- Symptoms appear with heavier exertion, not at rest
- Flare-ups are rare but more likely during viral infections or winter
Stage 1 is the turning point: with decisive action, you slow or almost flatten the rate of COPD decline; with denial, COPD progresses and the next stages hit harder.
6. COPD Symptoms by Stage
Doctors use GOLD stages and symptom scores to map COPD disease severity. Think of it as a framework rather than a rigid box; each person’s body expresses disease slightly differently.
6.1 Overview of COPD stages
GOLD uses:
- Spirometry (how much air you blow out)
- Symptom scores (breathlessness, flare-up history)
to group patients with chronic obstructive lung disease into categories.
For symptoms, a practical breakdown looks like this:
6.2 Stage 1 (Mild COPD)
Symptoms:
- Mild breathlessness with heavy exertion only
- “Smoker’s cough” that sticks around
- Slight wheeze with intense activity or colds
- No major limits in daily activities
Real-world example:
A 48‑year‑old construction worker smokes a pack a day. He walks miles on site but notices that he now breathes harder when carrying heavy tools upstairs. His cough “has been there for years.” Spirometry reveals early airflow obstruction—classic Stage 1.
6.3 Stage 2 (Moderate COPD)
Symptoms:
- Breathlessness with normal walking pace on flat ground
- Needing to stop to catch your breath when hurrying
- More frequent “bronchitis” episodes every winter
- Sleep disrupted after respiratory infections
- Fatigue at the end of the day
At this stage, many people with COPD finally seek help. They sense their chronic lung capacity changed in a real way.
Key feature of COPD here: Exercise capacity drops, and flare-ups increase. Untreated, this stage sets up acute exacerbations of COPD that send people to emergency rooms.
6.4 Stage 3 (Severe COPD)
Symptoms:
- Breathless with light activities such as dressing, showering, or light housework
- Very limited ability to walk more than a few minutes
- Recurrent acute exacerbations of COPD requiring steroids or hospital stays
- Marked fatigue and muscle weakness
- Weight loss and loss of appetite
- Anxiety or depression linked to breathing difficulties
Here, severe COPD takes over the rhythm of life. People plan around breathlessness, not around work or hobbies.
Complications associated with COPD in this stage can include:
- Pulmonary hypertension (high pressure in lung blood vessels)
- Right heart strain (cor pulmonale)
- Osteoporosis from steroids and inactivity
- High mortality in COPD if flare-ups stay uncontrolled
6.5 Stage 4 / End-Stage COPD
Sometimes called “very severe” COPD or end-stage COPD, this phase feels like lungs no longer meet the body’s basic needs.
Symptoms:
- Breathlessness even at rest, while sitting or talking
- Severe limitation of all physical activity
- Frequent acute COPD flares needing hospital care
- Possible need for long-term oxygen therapy
- Confusion or drowsiness from high carbon dioxide retention
- Marked weight loss and frailty
People with end-stage COPD are more likely to:
- Develop right-heart failure from chronic strain
- Experience frequent infections that spiral into respiratory failure
- Spend significant time hospitalized, which rapidly reduces quality of life
At this stage, teams focus on management of chronic obstructive pulmonary disease in a way that balances survival, comfort, and the person’s goals.
7. Severe COPD Symptoms: When the Disease Dominates Daily Life
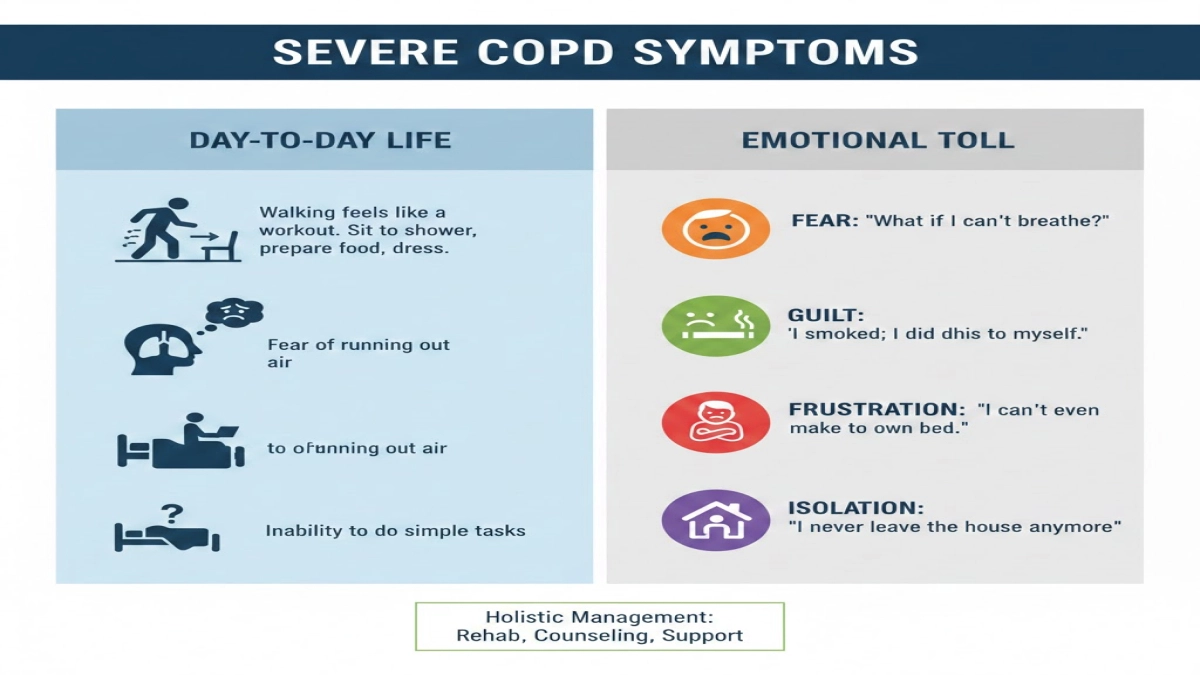
7.1 How severe COPD feels day to day
If you live with severe COPD, you already know this:
- Simply walking from the bedroom to the bathroom feels like a workout.
- You sit to shower, prepare food, and dress.
- You fear running out of air more than almost anything else.
Severe COPD symptoms include:
- Constant breathlessness, even at rest
- Needing oxygen for much of the day
- Inability to walk across a room without pausing
- Morning headaches from overnight carbon dioxide retention
- Trouble concentrating or thinking clearly
- Recurrent chest infections and COPD exacerbation events
- Swelling in legs from heart strain
These symptoms reduce quality of life in every domain: work, travel, intimacy, and social life. Many studies on burden of COPD confirm that advanced COPD ranks among the most limiting chronic diseases.
7.2 The emotional toll
Researchers and clinicians who work with people living with COPD hear the same themes:
- Fear: “What if I can’t breathe?”
- Guilt: “I smoked; I did this to myself.”
- Frustration: “I can’t even make my own bed.”
- Isolation: “I never leave the house anymore.”
A good management of chronic lung disease plan addresses symptoms and emotional health. Pulmonologists now recommend pulmonary rehabilitation, counseling, and peer support as core parts of treating COPD, not optional extras.
8. Red Flags of COPD: When to Act Fast
Some symptoms go beyond “bad day” and signal danger. These red flags of COPD require urgent or emergency care:
- Sudden or rapidly increasing breathlessness compared with your usual baseline
- Inability to speak full sentences because of shortness of breath
- Blue or gray lips, tongue, or fingertips
- New, severe chest pain, especially with breathlessness
- Confusion, extreme drowsiness, or agitation
- Very fast heartbeat or feeling like you might pass out
- No relief from your usual rescue inhaler or nebulizer
- Coughing up large amounts of thick, green, or bloody mucus
These signs point toward:
- An acute exacerbation of COPD
- Possible pneumonia or chronic respiratory infection
- Potential heart attack or pulmonary embolism
- Dangerous shifts in oxygen or carbon dioxide levels
Quick warning:
Do not “tough it out” at home when your breathing changes this way. Delaying care during a severe COPD flare increases the risk of death and long-term lung damage.
9. What Is One of the First Signs of COPD?
When researchers study the epidemiology of COPD and COPD prevalence in large populations, one feature stands out as a classic early clue:
A chronic cough with or without daily sputum in a person with a smoking or exposure history.
That simple combination – chronic cough plus risk factors – should always raise a flag.
Other early signs of COPD include:
- Getting out of breath when walking more quickly on level ground
- Wheezing during colds that lingers after others recover
- “Bronchitis every winter” that keeps returning
- Reduced exercise tolerance compared with a few years earlier
In any adult over 35–40 with these symptoms and causes in their background (smoking, biomass exposure, dusty workplaces), COPD should be considered and a pulmonary function test ordered.
Searches like “COPD may feel like tightness in my chest” reflect this early uncertainty. Many people do not realize that what they call “smoker’s cough” is by definition chronic bronchitis.
Remember:
Chronic bronchitis is defined as a cough with sputum production on most days for at least three months in two consecutive years. That pattern, combined with airflow obstruction on spirometry, places you squarely in the chronic bronchitis form of COPD.
10. How Doctors Diagnose COPD
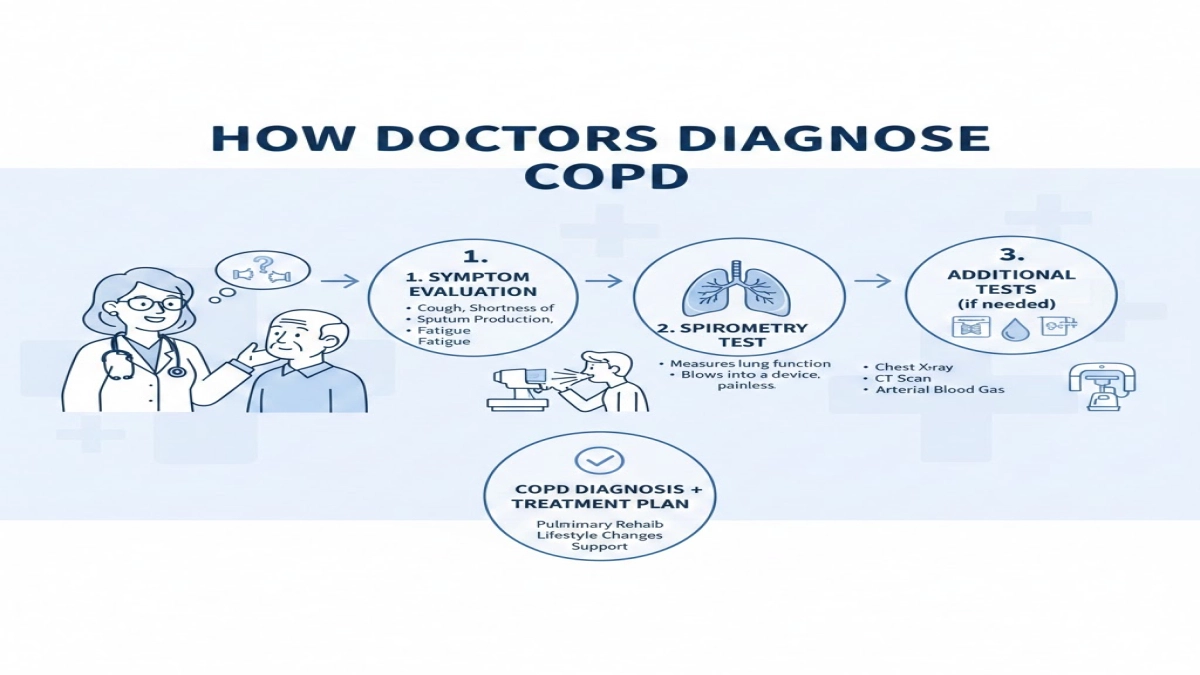
10.1 The core test: pulmonary function testing
To diagnose COPD, clinicians rely on:
- History and symptoms (chronic cough, breathlessness, exposures)
- Physical exam
- Pulmonary function test (spirometry)
Spirometry measures:
- How much air you blow out in one second (FEV1)
- How much air you blow out in total (FVC)
- The ratio FEV1/FVC
In COPD, the FEV1/FVC ratio drops and remains low even after a bronchodilator. This pattern confirms chronic obstructive lung disease.
No spirometry, no reliable diagnosis of COPD. Mislabeling asthma, heart failure, or COPD and interstitial lung disease as “just COPD” leads to the wrong treatments.
10.2 Other tests that support the diagnosis
Depending on your story, clinicians might also use:
- Chest X-ray or CT scan – to look for emphysema, masses, or chronic lung disease patterns
- Arterial blood gases – to assess oxygen and carbon dioxide levels
- Echocardiogram – to evaluate for pulmonary hypertension or right heart strain
These tools help distinguish asthma and COPD, pneumonia, heart failure, and other respiratory disease entities that share similar symptoms.
11. Living With COPD: Management That Actually Helps
You might be wondering, “Once I get COPD, what now? Is anything I do still worth it?”
The answer is yes. COPD treatments significantly improve symptoms and survival, even when COPD already feels advanced.
11.1 Core elements of COPD management
Evidence-based management of chronic obstructive pulmonary disease includes:
- Smoking cessation
- The most effective step to prevent COPD from getting worse
- When people quit, the decline in lung function slows dramatically
- Inhaled therapies
- Short-acting bronchodilators for quick relief
- Long-acting bronchodilators and inhaled steroids to reduce inflammation in COPD and keep airways open
- These treatments sit at the center of treating COPD in all modern guidelines
- Vaccination
- Flu, COVID-19, and pneumococcal vaccines reduce infections associated with COPD flare-ups.
- Pulmonary rehabilitation
- Structured pulmonary rehabilitation programs teach breathing techniques, exercise training, and energy-conservation strategies
- Research shows pulmonary rehabilitation reduces hospitalizations, improves walking distance, and boosts quality of life in people with stable COPD
- Oxygen therapy
- For advanced disease with low oxygen, home oxygen improves survival and comfort.
- Nutrition, exercise, and mental health care
- Targeted nutrition prevents muscle loss
- Tailored exercise counters deconditioning
- Counseling supports mental health, which COPD strongly affects
11.2 Stable COPD vs exacerbations
Clinicians divide life with COPD into:
- Stable COPD – symptoms fluctuate within a familiar range; no major infection or new strain
- Exacerbations – sudden worsening of breathlessness, cough, and sputum, often from infection or irritant exposure
People with people with stable COPD learn their baseline and monitor for changes. Having an “action plan” for flare-ups – when to increase inhalers, when to start steroids or antibiotics, when to seek emergency care – significantly lowers the risk of hospitalization.
11.3 A practical symptom-management checklist
Here’s a simple, real-world framework many respiratory teams use:
- Track your daily symptoms in a notebook or app.
- Note how far you walk on a “good day” vs a “bad day.”
- Learn your baseline peak flow or spirometry numbers if available.
- If you notice a trend toward more breathlessness or more sputum for several days, call your clinician before it becomes a crisis.
- Keep written instructions on what to do if your breathing suddenly changes – and share these with family members.
This stepwise approach gives you control, not just medication.
12. Can You Prevent COPD or Stop It From Getting Worse?
12.1 Who is at risk for COPD?
People who develop COPD share several features:
- Long smoking history or intense secondhand smoke exposure
- Long-term exposure to biomass smoke in poorly ventilated homes
- Decades working in dusty or chemical-heavy environments
- History of severe childhood lung infections
- Family history or genetic predispositions
Studies show people with COPD are more likely to have lower socioeconomic status, less access to primary care, and work in high-exposure jobs. These social factors explain why higher rates of COPD cluster in certain communities.
12.2 The best way to prevent COPD – and COPD from getting worse
The best way to prevent COPD from appearing or progressing:
- Never start smoking; quit if you currently smoke
- Insist on proper ventilation and protective masks in dusty or fume-heavy workplaces
- Reduce exposure to biomass fuels; use cleaner cooking options where possible
- Treat asthma aggressively to avoid long-term airway remodeling
- Seek early evaluation for persistent cough or breathlessness
From a public-health perspective, COPD in primary care settings requires earlier spirometry and education. GOLD and other initiative for chronic obstructive lung disease bodies stress that front-line clinicians should think about COPD as soon as a smoker reports a chronic cough.
13. The Bigger Picture: COPD, Other Lung Diseases, and Society
13.1 COPD and other lung diseases
Several conditions share overlapping symptoms with COPD:
- Asthma and COPD – Some people have features of both; this affects treatment choices.
- COPD and interstitial lung disease – Both cause breathlessness, but interstitial patterns on imaging and restrictive patterns on spirometry distinguish them.
- Heart failure – Another major condition related to COPD symptoms; it can mimic or coexist with COPD.
This complexity means clinicians must evaluate each person rather than assuming every smoker with breathlessness has COPD.
13.2 COPD in the United States and globally
When researchers examine COPD in the United States, they see:
- Millions living with diagnosed COPD
- Substantial numbers with undiagnosed disease
- Marked regional differences – rural areas and regions with coal mining or heavy industry show copd cases at higher levels
Globally, COPD is a major public-health challenge:
- The burden of COPD continues to rise, especially in low‑ and middle‑income countries.
- GOLD and similar groups track COPD prevalence and emphasize that COPD is a major cause of disability and death worldwide.
Across these populations, COPD is a lung disease that behaves as a systemic disorder. COPD affects muscles, metabolism, mood, and cardiovascular health. People with COPD also show higher rates of osteoporosis, depression, and ischemic heart disease associated with COPD.
14. Putting It All Together: Recognizing COPD Symptoms Early
Let’s connect the threads in a practical checklist.
If any of these describe you:
- You cough most days and bring up mucus, especially in the morning
- You feel more breathless than your same-age peers on stairs or hills
- You catch “bronchitis” almost every winter
- You have a long history of smoking or exposure to dust, fumes, or biomass smoke
…then COPD should be considered in your differential, even if you still work full-time and stay active.
Your next best steps:
- Book an appointment with your primary care clinician.
- State clearly: “I have a chronic cough and breathlessness. I smoked for years. I want a pulmonary function test to check for COPD.”
- Bring a written list of your symptoms, exposures, and how they changed over time – your history of COPD-like symptoms matters.
- Ask about referral to a pulmonologist and to a pulmonary rehabilitation program if COPD gets confirmed.
In my view, this is the most reliable path: respect your symptoms, push for testing, and then use modern management of COPD tools aggressively. COPD is a chronic condition and COPD is a long-term challenge, but it is not hopeless. Many people with COPD also return to walking programs, travel, and meaningful activities once they receive proper treatment and education.
People Also Ask: COPD Symptom FAQs
1. Can you have COPD without a cough?
Yes. Some people mainly feel breathless and tired and only have a mild or intermittent cough. A normal‑sounding cough does not rule out COPD; that is why spirometry remains critical.
2. How do I know if my cough is “just smoking” or COPD?
If you cough most days, especially in the morning, and you have smoked for years, you already meet the pattern for chronic bronchitis. When that pattern combines with airflow obstruction on spirometry, it becomes part of COPD. Do not wait for it to “go away” on its own.
3. Is COPD reversible if I quit smoking?
Damaged air sacs and scarred airways do not fully regenerate; COPD is permanent. However, quitting smoking immediately slows further damage, improves symptoms, and increases survival. Many people with stable COPD who quit regain better exercise capacity and experience fewer flares.
4. Can asthma turn into COPD?
Long-standing, poorly controlled asthma with continuous inflammation can remodel the airways and create fixed obstruction. In those cases, people receive diagnoses such as asthma–COPD overlap. Good asthma control in early years protects long-term lung function.
5. Do all smokers get COPD?
No. Genetics, environment, and infection history change individual risk. Still, research shows smokers remain far more likely to get COPD than non-smokers. When you remove smoking, COPD cases in a population drop dramatically.
6. Is there really no cure for COPD?
Current science does not offer a cure for COPD in the sense of fully restoring lung structure. But treatment—especially smoking cessation, inhalers, vaccination, and pulmonary rehab—changes the trajectory of life with COPD in a profound way.
7. Why does COPD sometimes get worse suddenly?
Infections, pollution spikes, or missed medications trigger sudden surges of airway inflammation and mucus, causing COPD exacerbation episodes. Each major flare can permanently reduce lung function, which explains why prevention and early treatment of infections matter so much.
Key Takeaways
- COPD is a progressive, chronic obstructive lung disease that blocks airflow and damages air sacs.
- Smoking represents the main cause of COPD, and COPD is largely preventable through smoking avoidance and clean air policies.
- Early COPD symptoms—chronic cough, daily sputum, and breathlessness on exertion—signal a window where aggressive treatment protects long-term function.
- Severe COPD symptoms include breathlessness at rest, frequent hospitalizations, and severe limitations in daily activities; these symptoms carry higher mortality in COPD.
- A pulmonary function test is essential to diagnose COPD accurately and distinguish it from other chronic lung disease entities.
- Combining inhalers, vaccination, smoking cessation, and pulmonary rehabilitation yields the best outcomes for people with COPD across all stages.
- If your breathing story matches what you read here, do not wait. Ask for spirometry, learn your numbers, and work with a clinician to build a personalized COPD action plan.
References
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2023 Report.
- World Health Organization. Chronic obstructive pulmonary disease (COPD) Fact Sheet. Updated 2023.
- Centers for Disease Control and Prevention (CDC). Chronic Obstructive Pulmonary Disease (COPD). Data and Statistics.
Medical Disclaimer
Information on this website is for general education only. It is not medical advice.
The content on COPD.MEDLIFEGUIDE is written to help people understand COPD and other breathing conditions in a clear and simple way. It is not a substitute for professional medical care, diagnosis, or treatment.
Always talk to a licensed healthcare provider for personal medical concerns.
Do not ignore symptoms or delay getting help because of something you read on this site. If you think you may be having a medical emergency, call your local emergency number right away.
Leave a Reply