
COPD Stages in 2025: What Each Stage Really Means for Your Life
Doctors classify chronic obstructive pulmonary disease (COPD) into four stages – mild, moderate, severe, and very severe – based mainly on how much air you can blow out in one second on a pulmonary function test (spirometry).
- Stage 1 (mild) – Symptoms of COPD stay light: a chronic cough, mild breathlessness, normal daily activity.
- Stage 2 (moderate) – Breathlessness appears with routine tasks like walking or stairs. This stage brings many first diagnoses of COPD.
- Stage 3 (severe) – Symptoms limit daily life, COPD exacerbation risk rises, and quality of life drops without strong management.
- Stage 4 (very severe) – Very limited lung function, frequent acute exacerbations of COPD, and high mortality in COPD without intensive care.
Research shows that COPD is a progressive, long-term lung disease, but people with COPD who quit smoking, follow a tailored COPD treatment plan, and join a pulmonary rehabilitation program slow how fast COPD progresses and live better, longer lives.
Quick Summary
- COPD = chronic obstructive pulmonary disease, a chronic lung disease that blocks airflow and makes breathing hard.
- Main cause of COPD worldwide: smoking, but air pollution, occupational dusts, and genetics also cause COPD.
- Doctors use the GOLD classification (Global Initiative for Chronic Obstructive Lung Disease) to describe four stages based on lung function.
- Common symptoms of COPD include: chronic cough, mucus, breathlessness, chest tightness, frequent infections, and fatigue.
- Stage 4 COPD = very severe COPD with very low lung function, serious symptoms, and higher mortality in COPD.
- The rate of COPD progression depends on smoking status, treatment quality, exacerbation frequency, nutrition, exercise, and co‑existing diseases.
- Weight loss usually appears in later stages and signals higher risk, but targeted nutrition and exercise improve strength and survival.
- No cure for COPD exists today; COPD is permanent, but smart management of COPD dramatically improves quality of life.
Keep reading, because the next sections show exactly how doctors diagnose COPD, how each stage feels in real life, and what you can do today to stop COPD getting worse.
Key Points
- COPD is a major chronic respiratory disease and ranks among the top three causes of death worldwide.
- COPD is a lung disease that includes emphysema and chronic bronchitis as the two most common types of COPD.
- The biggest risk factor for COPD remains tobacco smoking, but not every smoker will get COPD.
- A simple pulmonary function test (spirometry) in primary care detects COPD years before severe symptoms appear.
- Pulmonary rehabilitation and exercise stand among the most effective COPD treatments for all COPD stages.
- People with stable COPD who stick with a plan experience fewer hospital visits, stay active, and protect independence.
1. Why COPD Staging Matters So Much In 2025
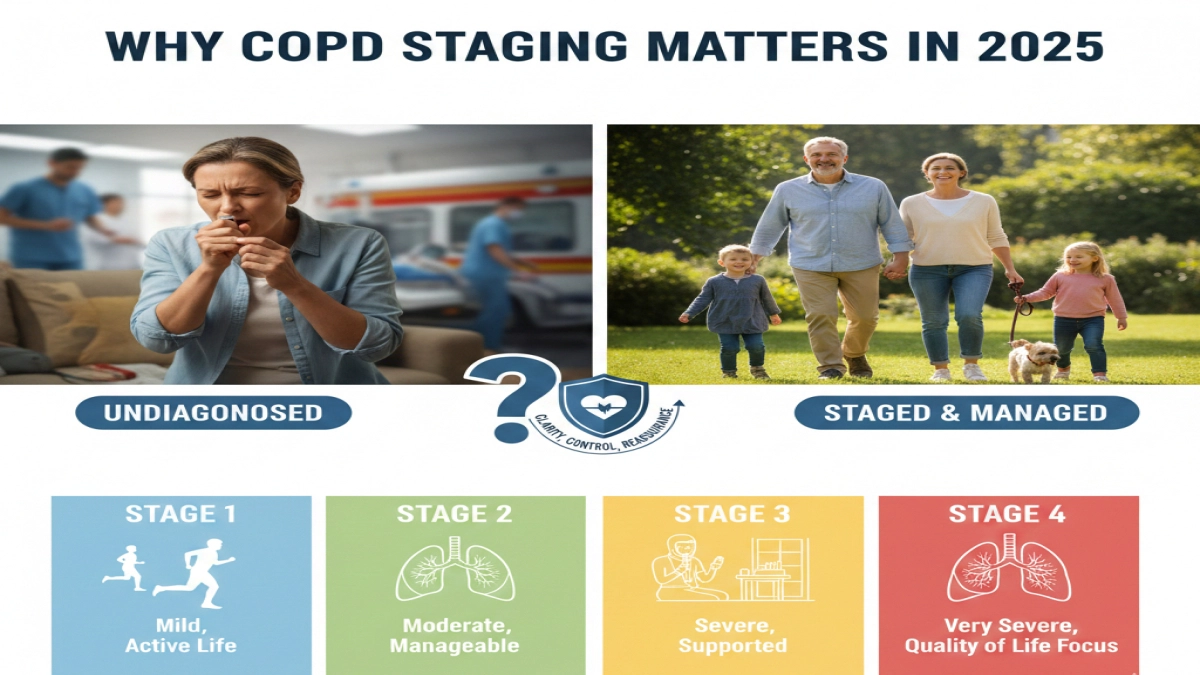
A surprising fact: in many countries, up to half of all cases of COPD remain undiagnosed until people land in the emergency room with an acute COPD flare.
By that time, their lungs already lost a large share of function.
COPD in the United States and worldwide places a massive burden on families and health systems. The burden of COPD includes medical costs, missed work, disability, and lost independence. Yet COPD is largely preventable and highly manageable when you understand:
- Which COPD stage you fall into
- What that stage means for your lungs and life expectancy
- Exactly which steps slow the development of COPD and prevent COPD from getting worse
Searchers who type “COPD stages” usually want three things at once:
- Clarity – “Where am I on this scale? Is my COPD worse than I think?”
- Control – “What can I do right now to slow COPD progression?”
- Reassurance – “Does life still look okay after a COPD diagnosis?”
This guide answers those questions in plain language, backed by the Global Initiative for Chronic Obstructive Lung Disease (GOLD), major studies, and real‑world experience from people living with COPD.
Stay with this article, and by the end you will:
- Understand each COPD stage in human terms
- Know which tests your doctor uses to diagnose COPD and stage it
- See what daily life can look like at Stage 1 vs Stage 4
- Learn practical steps to improve your quality of life at every stage
The next section starts with the basics: What exactly is this disease that so many people call “just smoker’s lung”?
2. What Is COPD?
A. Definition And Causes
Chronic obstructive pulmonary disease (COPD) is a chronic obstructive lung disease where the airways narrow, the lung sacs lose elasticity, and ongoing inflammation in COPD blocks airflow in and out of your lungs.
Doctors group two main conditions under COPD:
- Emphysema – damage to the tiny air sacs (alveoli)
- Chronic bronchitis – long‑lasting inflammation of the airways
- Classic teaching says: chronic bronchitis is defined as a productive cough for at least three months per year, for two consecutive years
Together, emphysema and chronic bronchitis form the most common types of COPD.
Main cause of COPD and common causes of COPD
Research and epidemiology of COPD show a clear pattern:
- Smoking stands as the main cause of COPD and the biggest risk factor for COPD
- Other common causes of COPD and risk factors include:
- Indoor and outdoor air pollution
- Dusts and fumes at work (mining, construction, metal work, agriculture)
- Biomass fuel smoke from cooking or heating
- Childhood lung infections and chronic respiratory problems
- Genetics such as alpha‑1 antitrypsin deficiency
People who smoke or live with heavy pollution are more likely to develop COPD earlier and progress faster. Yet not every smoker will get COPD, which frustrates many patients and families. Genetics, early life exposures, and repeated infections interact in complex ways during the development of COPD.
B. Symptoms And Impact On Daily Life
Doctors describe symptoms and causes of COPD in textbooks. Patients describe a very different reality:
- Chronic cough that “never goes away”
- Mucus (phlegm) that forces a person to clear their throat repeatedly
- Breathlessness when talking, climbing stairs, or walking uphill
- Wheezing, chest tightness, noisy breathing
- Frequent chest infections and acute exacerbations of COPD
- Exhaustion after simple tasks, trouble sleeping flat, weight changes
In early stages, signs of COPD feel easy to dismiss:
“I just got older.”
“Must be that cold I never fully shook.”
“It’s my weight, not my lungs.”
As COPD progresses, symptoms of COPD squeeze daily life tighter:
- People with COPD skip social events because they feel embarrassed by coughing
- Many people with COPD also avoid walking with friends because they fear slowing everyone down
- Hobbies disappear – gardening, dancing, playing with grandkids – replaced by recovery breaks in a chair
This erosion of quality of life matters as much as the numbers on a test. So how do doctors measure and stage this chronic lung disease?
The next section explains how many stages of COPD exist and which numbers define them.
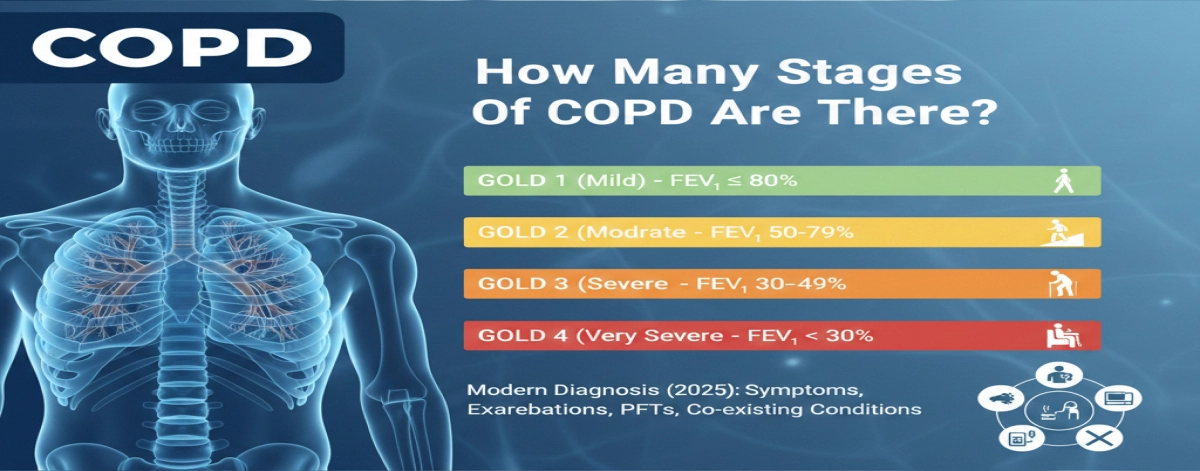
3. How Many Stages Of COPD Are There?
A. Explanation Of The Four Stages
Specialists describe four stages of COPD based mainly on pulmonary function measured with a spirometer. This simple pulmonary function test asks you to blow out as hard and fast as possible.
Key number: FEV₁ – Forced Expiratory Volume in 1 second
Doctors compare your FEV₁ to the “predicted” value for your age, sex, and height.
Using the Global Initiative for Chronic Obstructive Lung Disease (GOLD) system (Global Initiative for Chronic Obstructive; Initiative for Chronic Obstructive Lung Disease), they classify airflow limitation as:
- GOLD 1 (Mild) – FEV₁ ≥ 80% predicted
- GOLD 2 (Moderate) – FEV₁ 50–79% predicted
- GOLD 3 (Severe) – FEV₁ 30–49% predicted
- GOLD 4 (Very Severe) – FEV₁ < 30% predicted
You can think of these four groups as Stage 1–4.
B. Brief Overview Of The Classification System
Doctors do not look only at spirometry. A modern diagnosis of COPD and staging in 2025 includes:
- Symptoms – breathlessness scores, cough frequency
- Exacerbation history – number of flare‑ups or hospital stays in the last year
- Pulmonary function test results
- Co‑existing conditions – heart disease, pulmonary hypertension, asthma and COPD overlap, interstitial lung disease, obesity, depression
Guidelines from GOLD and national societies state that COPD should be considered in any adult with:
- Chronic cough or sputum
- History of exposure to smoke or fumes
- Breathlessness on exertion
- And airflow limitation on spirometry
Next, let’s break down each stage so you can recognize where you or your loved one fits and what to do about it.
4. Detailed Breakdown Of The Four Stages Of COPD
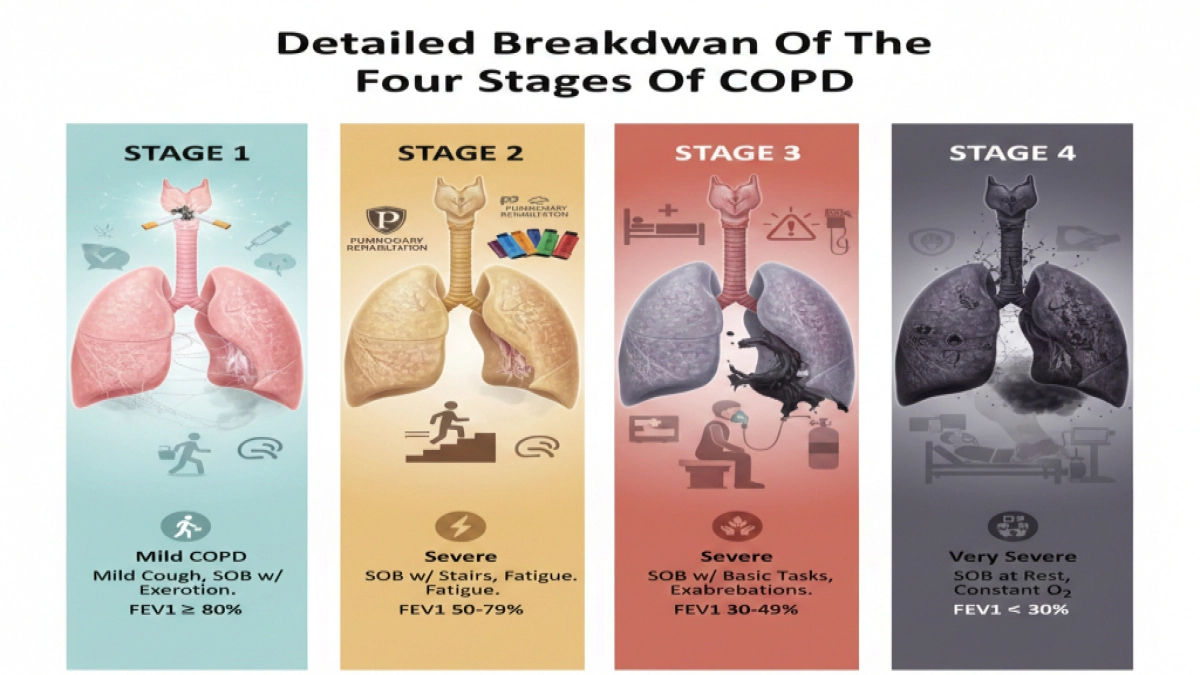
A. Stage 1: Mild COPD
1. Symptoms And Diagnosis
In Stage 1, COPD symptoms stay subtle:
- Chronic cough with light sputum
- Mild shortness of breath with heavy exertion
- Occasional wheeze during colds
- Many people with stable COPD at this stage feel “basically fine”
Here’s a typical case:
A 52‑year‑old office worker smokes a pack a day.
He notices a daily morning cough and needs to stop once on a long flight of stairs.
He blames “being out of shape”.
A routine check shows reduced airflow. Spirometry confirms mild COPD.
Doctors diagnose COPD when:
- Spirometry shows a reduced FEV₁/FVC ratio (airflow obstruction)
- FEV₁ stays ≥ 80% of predicted
2. Treatment Options And Management
For Stage 1, the best way to prevent COPD from getting worse starts with aggressive risk‑factor control:
- Stop smoking – the single most effective step to protect remaining lung function
- Reduce exposure to dust, fumes, biomass smoke
- Get influenza and pneumococcal vaccines
COPD treatments at this stage usually include:
- Short‑acting bronchodilator inhaler as needed
- Education on inhaler technique
- Early referral to a pulmonary rehabilitation program when symptoms disturb daily life
Doctors focus heavily on management of chronic obstructive pulmonary disease early, because COPD is a progressive disease and the slope of decline starts here.
Mini‑hook: If Stage 1 looks manageable, Stage 2 reveals why most COPD cases first get diagnosed there.
B. Stage 2: Moderate COPD
1. Symptoms And Diagnosis
In Stage 2, COPD symptoms step into the foreground:
- Breathlessness when climbing one flight of stairs
- Slowing down when walking with friends
- Noticeable fatigue in the evening
- Chronic cough and sputum feel routine
Many people with COPD reach this stage before anyone orders a pulmonary function test. COPD in primary care sometimes gets mistaken for “aging”, asthma, or being out of shape.
Research on the epidemiology of COPD shows that COPD prevalence rises sharply after age 40, with higher rates of COPD in smokers, in low‑income regions, and in people exposed to biomass smoke.
At Stage 2:
- Spirometry confirms airflow obstruction
- FEV₁ measures 50–79% of predicted
Doctors check for other respiratory disease and chronic respiratory problems, including:
- Asthma and COPD overlap (ACO)
- Bronchiectasis
- Early interstitial lung disease
2. Treatment Options And Management
For Stage 2, the treatment plan expands:
- Long‑acting bronchodilators
- Inhaled corticosteroids in selected patients with frequent exacerbations
- Structured pulmonary rehabilitation – supervised exercise, breathing techniques, education
- Weight and nutrition assessment
- Strength and endurance training
In my view, pulmonary rehabilitation offers one of the most underrated tools for people living with COPD. I see a pattern in patient stories:
Before rehab: “I felt scared to move because any breathlessness seemed dangerous.”
After rehab: “I learned safe limits and pushed them in a controlled way. My confidence and stamina increased.”
Experts in management of COPD recommend pulmonary rehab at Stage 2, not as a last resort. People with stable COPD who train their muscles, learn pacing, and understand inhaler use cut their risk for COPD exacerbation and hospitalization significantly.
Mini‑hook: When COPD progresses into Stage 3, the disease stops feeling like an inconvenience and starts to control the calendar.
C. Stage 3: Severe COPD
1. Symptoms And Diagnosis
Stage 3 signals severe COPD. This stage changes daily life:
- Breathlessness during basic tasks – showering, dressing, walking across a room
- Need to rest on the way from bedroom to kitchen
- Sleep disruption and anxiety about breathing at night
- More frequent acute exacerbations of COPD – flare‑ups triggered by infections or pollution
- Loss of work ability, social isolation, depression
At this stage, patients with chronic obstructive lung disease frequently see specialists. Tests often reveal:
- FEV₁ between 30–49% predicted
- Signs of pulmonary hypertension (high pressure in lung vessels)
- Right‑sided heart strain in some cases
- Lower oxygen levels during exertion
Doctors track these numbers because they relate directly to mortality in COPD and future risk.
2. Treatment Options And Management
Stage 3 treatment becomes multi‑layered:
- Combination long‑acting bronchodilators
- Inhaled steroids when appropriate
- Repeated, structured pulmonary rehabilitation program cycles
- Oxygen therapy for those with low resting or exertional oxygen saturation
- Vaccinations, early antibiotics and steroids for acute COPD flares
- Mental health support and social work input
At this point, COPD increases risk of:
- Lung infections
- Blood clots
- Heart failure
- Metabolic issues and weight loss
A key feature of COPD at Stage 3: the body spends energy simply to breathe. People with COPD often lose muscle and weight without planning to.
A quick warning: Never ignore a sudden spike in breathlessness, blue lips or fingers, or confusion. Treat this as an emergency and seek care immediately.
Mini‑hook: Stage 4 COPD raises the stakes even higher, but it also clarifies which actions protect comfort and dignity most.
D. Stage 4: Very Severe COPD
1. Symptoms And Diagnosis
Stage 4 means very severe COPD. COPD affects nearly every part of daily life:
- Shortness of breath at rest or with minimal movement
- Need for oxygen most or all of the day
- Frequent, sometimes monthly, hospitalizations for acute exacerbations of COPD
- Severe fatigue, weight loss, and muscle wasting
- Anxiety and fear around every breath
Doctors document:
- FEV₁ < 30% of predicted
- Strong limitation on exercise tests
- High risk of pulmonary hypertension and right‑sided heart failure
- Possible overlap with other conditions such as COPD and interstitial lung disease
Many people with COPD also live with heart disease, diabetes, or kidney disease at this stage, which complicates treatment.
2. Treatment Options And Management
Management of Stage 4 focuses on:
- Maximizing comfort and function
- Reducing hospital visits
- Aligning treatment with patient values and goals
Care elements usually include:
- Optimized inhaler and nebulizer regimens
- Long‑term oxygen therapy
- Non‑invasive ventilation for some patients (e.g., CPAP/BiPAP)
- Advanced pulmonary rehabilitation adapted to limitations
- Palliative care input for symptom relief and advance care planning
- Evaluation for lung volume reduction surgery or lung transplantation in selected patients
Here, management of chronic symptoms becomes as important as treating COPD directly. Breathlessness relief, anxiety control, sleep, and caregiver support matter deeply.
Experts highlight that COPD is a chronic, long‑term disease and COPD is permanent, but COPD treatments and support still change the course of daily life, even at Stage 4.
5. COPD Stages And Life Expectancy

A. How COPD Stages Affect Life Expectancy
Researchers measure mortality in COPD using large population studies and tools like the BODE index (Body‑mass, Obstruction, Dyspnea, Exercise capacity). They consistently show:
- Lower FEV₁ (higher stage) links to higher mortality in COPD
- More frequent exacerbations predict higher risk
- Weight loss, especially muscle loss, signals worse outcomes
Put simply:
- Earlier stages (1–2) – Many people live for decades with good quality of life when they stop smoking and follow treatment
- Later stages (3–4) – Risk rises, but outcomes still vary widely based on management, comorbidities, and social support
Important nuance: COPD is a major cause of death, yet many people with COPD are more likely to die from heart disease, infections, or cancers related to COPD and shared risk factors such as smoking.
B. Factors Influencing Prognosis
Life expectancy depends on more than stage alone. Key influences:
- Smoking status – Continuing to smoke accelerates decline; quitting slows it dramatically
- Exacerbations – Each severe exacerbation damages the lungs and increases future risk
- Weight and muscle mass – Underweight status and muscle wasting worsen survival
- Comorbidities – Heart disease, diabetes, osteoporosis, anxiety, depression
- Activity level – Regular movement and exercise through pulmonary rehabilitation improve survival
- Adherence – Taking medications correctly and completing rehab programs matters
Studies show that people with stable COPD who:
- Quit smoking
- Stay active
- Maintain a healthy weight
- Use inhalers correctly
live significantly longer than COPD patients with the same lung function who do not follow those steps.
Mini‑hook: Life expectancy creates important questions, but for many readers the more urgent question is: “What exactly does Stage 4 look like day to day, and how do we handle it?”
6. Understanding Stage 4 COPD
A. Characteristics And Symptoms Of Stage 4
Stage 4, or very severe COPD, brings:
- Breathlessness at rest
- Dependency on oxygen
- Inability to walk far without stopping
- Difficulty speaking in full sentences
- Frequent acute COPD flare‑ups triggered by minor infections or weather changes
- Possible confusion or headaches from high carbon dioxide levels
Families often describe this phase as a series of crises:
Hospital stay.
A few stable weeks at home.
Another infection, another ambulance ride.
Doctors view Stage 4 as the phase where COPD progresses into advanced, life‑limiting illness. Many complications become associated with COPD at this point:
- Pulmonary hypertension
- Right heart failure
- Severe weight loss and cachexia
- Osteoporosis and fractures
- Depression and anxiety
B. Management And Care Considerations
Effective care at Stage 4 balances longer life with better life.
Core goals:
- Ease breathlessness
- Reduce COPD exacerbation frequency and severity
- Support caregivers
- Plan ahead for medical decisions
Key components:
- High‑intensity inhaler therapy
- Oxygen titrated to safe levels
- Breathing techniques (pursed‑lip breathing, positions of ease)
- Short courses of steroids and antibiotics for flares
- Early palliative care involvement (not only at end of life)
- Honest conversations about resuscitation, intubation, and preferred place of care
In this stage, COPD is a long‑term disease, yet priorities shift from purely “treating COPD” to living as well as possible despite it.
7. How Quickly Does COPD Progress?
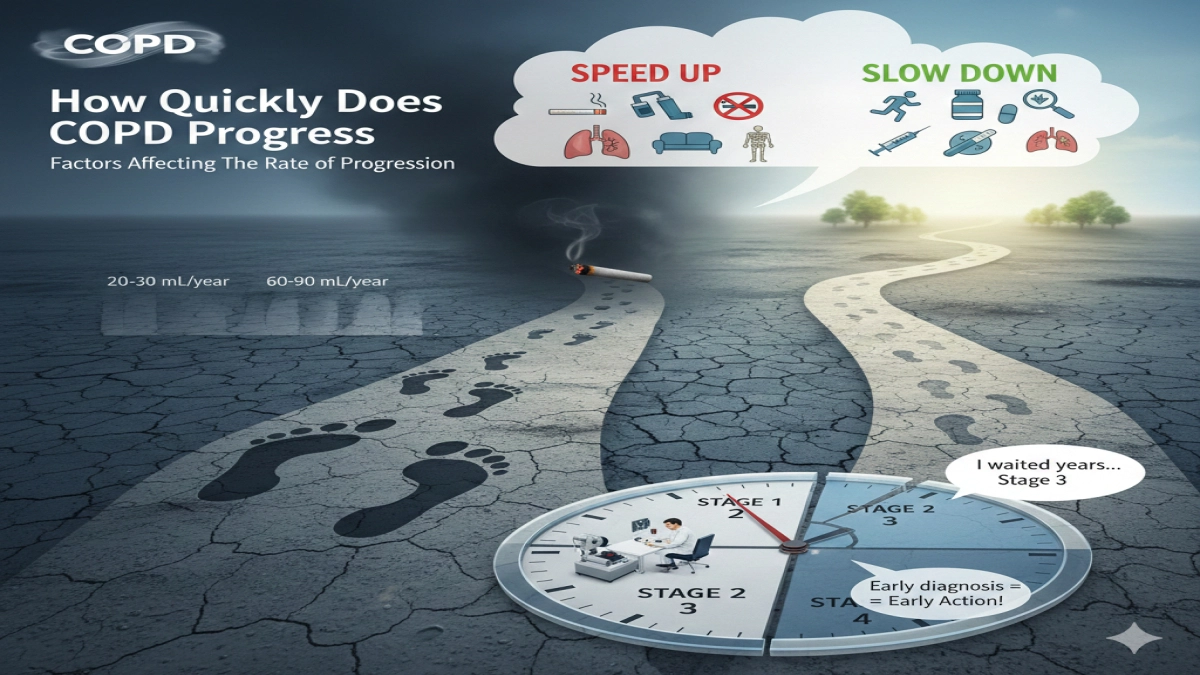
A. Factors Affecting The Rate Of Progression
The rate of COPD progression varies between individuals. Data from large cohorts show:
- Healthy nonsmokers lose about 20–30 mL of FEV₁ per year after mid‑life
- Smokers with COPD can lose two to three times that amount yearly when they keep smoking
- Quitting smoking slows decline back toward the normal curve
Factors that speed up progression:
- Continuing to smoke
- Repeated acute exacerbations of COPD
- Poor inhaler technique
- Low physical activity
- Malnutrition
- Uncontrolled comorbidities (e.g., heart failure)
Factors that slow progression:
- Early diagnosis of COPD with spirometry
- Complete smoking cessation
- Regular pulmonary rehabilitation and exercise
- Correct medication use
- Up‑to‑date vaccinations
- Prompt treatment of infections
From the perspective of epidemiology of COPD, populations with strong clean‑air regulations, smoking control, and primary care screening show lower COPD prevalence and slower rate of COPD progression at the population level.
B. Importance Of Early Diagnosis And Intervention
Here is a mistake I see repeatedly in stories from people living with COPD:
“I waited years to test my lungs because I feared the result.
When I finally went, my doctor said I had Stage 3 COPD.”
A five‑minute pulmonary function test in a doctor’s office catches airflow limitation early. Early detection allows:
- Strong prevention of further damage
- Early management of chronic obstructive pulmonary disease with lifestyle changes and medications
- Planning for work, retirement, and family roles before severe limits appear
Healthcare experts emphasize COPD in primary care: when family doctors test any patient with chronic cough or breathlessness, they catch more cases of COPD at Stage 1 and Stage 2 instead of Stage 3 and Stage 4.
Mini‑hook: Once COPD reaches advanced stages, weight loss and muscle wasting step in as silent but powerful players in prognosis.
8. Weight Loss And COPD Stages
A. When Weight Loss Typically Begins
Significant weight loss rarely appears in mild COPD. It tends to show up:
- In severe COPD (Stage 3) and very severe COPD (Stage 4)
- After repeated hospitalizations and flares
- In people who feel too breathless to cook, eat, or shop
Doctors call this COPD cachexia – a combination of:
- Higher resting energy use (breathing harder, using accessory muscles)
- Inflammation in COPD that drives muscle breakdown
- Loss of appetite and taste changes
- Depression and fatigue
Studies link low body weight and low muscle mass to higher mortality in COPD. In simple terms: weight loss at later stages signals higher risk.
B. Impact Of Weight Loss On Health And Management
Unplanned weight loss leads to:
- Weak respiratory muscles
- Higher risk of infection
- Poor wound healing
- Difficulty participating in pulmonary rehabilitation
To counter this, guidelines on management of chronic lung disease recommend:
- High‑protein, energy‑dense diets
- Small, frequent meals to reduce breathlessness while eating
- Nutritional supplements when needed
- Strength training as part of pulmonary rehabilitation program design
A short case example:
Maria, 67, reached Stage 3 COPD.
Over a year she lost 10 kg without trying and felt too tired to prepare meals.
Her care team added a dietitian, adjusted her inhalers, and enrolled her in rehab.
With targeted nutrition and exercise, her weight stabilized and she regained leg and arm strength, which reduced breathlessness during everyday tasks.
Experts on management of COPD treat nutrition and exercise as core therapy, not a side note.
9. Living With COPD: Practical Coping Strategies
You can live a full, meaningful life at every stage of COPD. The key lies in practical systems rather than willpower alone.
A. Lifestyle Changes And Management Techniques
1. Stop smoking and avoid irritants
- Treat smoking as the central risk factor for COPD that you control
- Use nicotine replacement, medications, and counseling
- Avoid secondhand smoke and indoor pollutants
2. Move daily within your limits
Many people with COPD fear exercise. Research shows that treating COPD with structured exercise through rehab:
- Improves exercise tolerance
- Reduces breathlessness
- Lowers hospital admission risk
Even on your own, you can:
- Walk indoors with rest breaks
- Use light hand weights or resistance bands
- Practice sit‑to‑stand repetitions from a sturdy chair
3. Master breathing techniques
Pulmonary rehab specialists teach techniques that help during breathless spells:
- Pursed‑lip breathing
- Diaphragmatic breathing
- Forward‑leaning positions
I strongly recommend learning these early, not waiting for severe COPD.
4. Create a written COPD action plan
Work with your clinician to define:
- Green zone – stable COPD: what “good days” look like and what you do
- Yellow zone – early flare‑up signs: increased cough, sputum, breathlessness
- Red zone – emergency signs
Research shows that people with COPD often delay treatment of flares by several days. A written plan shortens this delay and reduces hospital visits.
B. Support Systems And Resources
Living with chronic lung disease drains emotional reserves. Strong support transforms the journey.
Useful supports:
- Local pulmonary rehabilitation and exercise groups
- Peer support groups for people living with COPD and caregivers
- Respiratory nurse or educator visits
- Telehealth follow‑ups for medication and inhaler checks
In my experience reading patient narratives, those who build a “COPD care team” – family, clinicians, rehab staff, peers – handle crises better and feel less alone.
10. Conclusion – Living Well With A Chronic Lung Disease
Here is the honest summary:
- COPD is a lung disease that does not reverse; COPD is permanent and COPD is a chronic, long‑term condition.
- COPD is a progressive disease, yet the speed of that progression sits heavily in your hands and your care team’s hands.
- COPD is largely preventable through smoking control and clean air, and highly manageable through evidence‑based care.
From a big‑picture view, COPD is a major public‑health challenge, with millions of COPD cases worldwide and a heavy burden of COPD on families and systems.
From an individual view, COPD affects:
- How you breathe
- How you move
- How you connect with people you love
The unique value of understanding COPD stages lies here: once you know your stage and your risks, you can stop guessing and start planning.
Use this article as a checklist when you talk with your clinician:
- Clarify your stage with a recent pulmonary function test
- Review your action plan to prevent COPD flares
- Ask for a referral to pulmonary rehabilitation
- Address weight, mood, and sleep – not just inhalers
No cure for COPD exists right now. At the same time, millions of people with COPD around the world prove every day that you can adapt, protect your quality of life, and stay in charge of your story.
People Also Ask – COPD Stages FAQ
1. What are the 4 stages of COPD?
Doctors use GOLD stages based on spirometry:
- Stage 1 (mild): FEV₁ ≥ 80% predicted
- Stage 2 (moderate): 50–79%
- Stage 3 (severe): 30–49%
- Stage 4 (very severe): < 30%
They combine this with symptoms, exacerbation history, and other conditions to guide treatment.
2. Can you stop COPD from getting worse?
You cannot reverse structural lung damage, but you can slow COPD progression dramatically. Smoking cessation, correct inhaler therapy, vaccinations, pulmonary rehab, exercise, and early flare treatment stand as the most effective ways to stop COPD worse outcomes and protect remaining function.
3. How long can you live with Stage 4 COPD?
Life expectancy in Stage 4 varies widely. It depends on lung function, exacerbation frequency, nutrition, heart function, and comorbidities. Some people survive years with strong support; others decline faster. Your doctor can estimate risk using tools like the BODE index and tailor plans to your situation.
4. Does every smoker get COPD?
No. Many smokers never develop COPD, while some non‑smokers do. However, smoking raises the risk for COPD several‑fold and explains most cases of COPD worldwide. Genetics, early life events, and exposures such as dust and biomass smoke shape who will develop COPD.
5. Is COPD reversible if caught early?
COPD damage does not fully reverse. However, early detection and treatment stabilize lung function, improve symptoms, and prevent rapid decline. In that sense, early‑stage COPD behaves more controllably than many people expect.
6. What is the difference between asthma and COPD?
Asthma usually starts earlier in life, shows more variable symptoms, and responds strongly to bronchodilators and steroids. COPD usually appears after long‑term exposure to smoke or irritants, and airflow limitation stays more fixed. Some people show features of both – called asthma and COPD overlap – which requires tailored management.
7. How does COPD relate to other diseases?
Many conditions come associated with COPD, including heart disease, lung cancer, osteoporosis, depression, anxiety, and infections. COPD increases the risk of these problems through shared risk factors (like smoking) and chronic inflammation.
References
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of COPD. 2023 Report.
- World Health Organization. Chronic obstructive pulmonary disease (COPD) fact sheet.
- Centers for Disease Control and Prevention (CDC). Chronic Obstructive Pulmonary Disease (COPD).
Medical Disclaimer
Information on this website is for general education only. It is not medical advice.
The content on COPD.MEDLIFEGUIDE is written to help people understand COPD and other breathing conditions in a clear and simple way. It is not a substitute for professional medical care, diagnosis, or treatment.
Always talk to a licensed healthcare provider for personal medical concerns.
Do not ignore symptoms or delay getting help because of something you read on this site. If you think you may be having a medical emergency, call your local emergency number right away.