
COPD Causes Explained: From Smoking and Pollution to Flare-Up Triggers
Quick summary
If you want the short answer before you scroll:
- COPD is a lung disease that blocks airflow and makes breathing feel like “trying to inhale through a straw.”
- Smoking stands as the main cause of COPD worldwide, yet up to one third of COPD cases occur in people who never smoked.
- Key causes of COPD include cigarette smoking, secondhand smoke, indoor and outdoor air pollution, workplace dust and chemicals, and genetic factors such as alpha‑1 antitrypsin deficiency.
- Common symptoms of COPD include chronic cough, mucus, shortness of breath on exertion, chest tightness, and frequent chest infections.
- COPD exacerbation or flare-ups usually start with infections or exposure to cold air, smoke, or pollution, and they push many patients into the emergency department.
- You prevent COPD or slow COPD progression mainly by quitting smoking, reducing exposure to lung irritants, staying vaccinated, and joining a structured pulmonary rehabilitation program.
- No current cure for COPD exists. COPD is permanent in the sense that damaged air sacs do not regrow, yet treating COPD early changes the entire trajectory of the disease and protects quality of life.
Keep reading if you want a clear, practical map of every major cause and trigger, plus what you need to change right now to protect your lungs.

Key points at a glance
- COPD is a chronic obstructive pulmonary disease and a leading cause of chronic respiratory disease and death worldwide.
- COPD is a lung condition that is largely preventable. Research shows that smoking and polluted air explain most cases of COPD.
- Common types of COPD include emphysema and chronic bronchitis. Chronic bronchitis is defined as a productive cough for at least three months per year across two consecutive years.
- COPD affects more than 300 million people globally and creates a heavy burden of COPD for families and health systems.
- People with COPD are more likely to face hospital admissions, pulmonary hypertension, heart disease, and depression.
- Doctors diagnose COPD with a pulmonary function test (spirometry) that measures pulmonary function and airflow obstruction.
- The best way to prevent COPD and keep COPD from getting worse: quit smoking, avoid smoke-filled and dusty environments, stay consistent with inhalers, and complete pulmonary rehabilitation.
- COPD should be considered in anyone over 40 with a long history of COPD risk factors such as smoking or biomass exposure plus breathlessness or chronic cough.
If you live with chronic cough, breathlessness, or you care for people living with COPD, this next part matters, because it explains exactly how COPD develops in the first place.
1. Introduction: why COPD causes matter more than the label
You can treat breathlessness with inhalers. You can give oxygen. You can rush someone with acute COPD symptoms to the emergency department.
If you ignore what actually caused their chronic lung disease, though, the cycle repeats.
Research from the Global Initiative for Chronic Obstructive Lung Disease and the World Health Organization shows that COPD is a major driver of death and disability worldwide. COPD ranks among the top three causes of death globally and drives huge costs in hospitalizations, lost work, and reduced quality of life.
In the United States, COPD in the United States leads to tens of thousands of deaths each year and affects millions. Many of those people never received a clear explanation of why their lungs failed.
You might even know someone who says, “I just got old,” when in reality, decades of preventable exposure created a chronic obstructive lung disease that now blocks every breath.
So let us start with what COPD actually is, then drill down into the symptoms and causes, step by step.
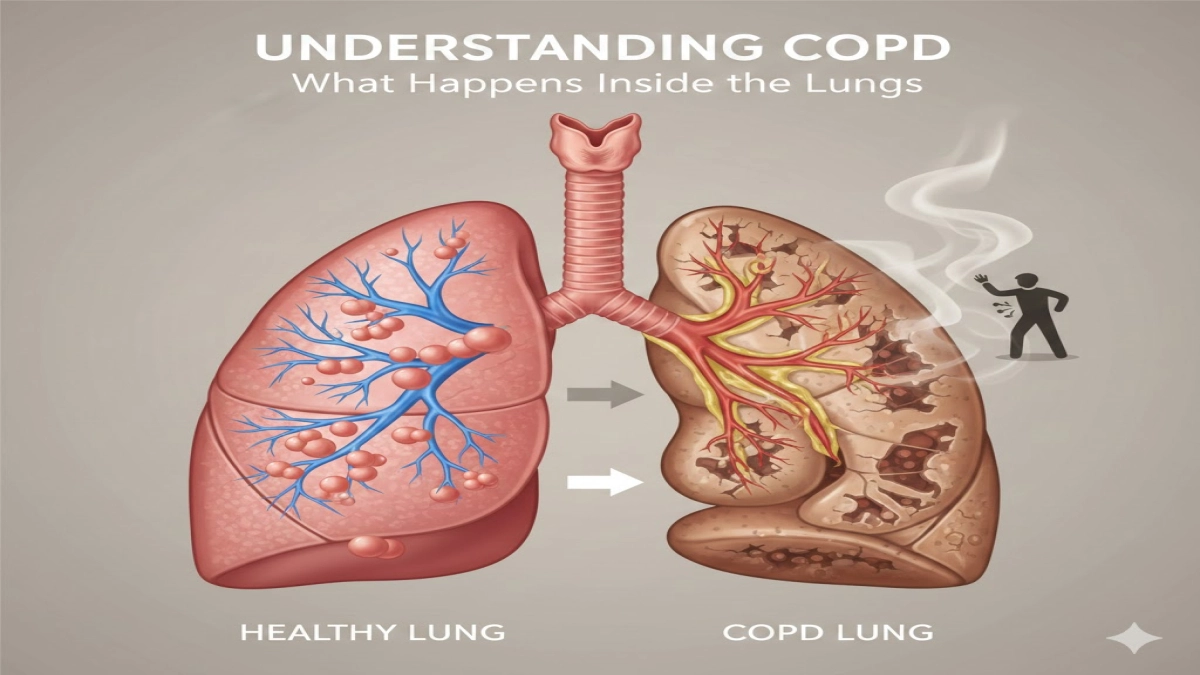
2. Understanding COPD: what actually happens inside the lungs
COPD in plain language
COPD is a chronic lung condition that narrows the airways and destroys the tiny air sacs that deliver oxygen to the blood. Doctors classify it as a chronic obstructive pulmonary disease because airflow stays blocked even after you use a bronchodilator.
Think of healthy lungs as a tree full of flexible branches and millions of tiny balloons.
In COPD:
- The airways stay inflamed and clogged with mucus.
- The tiny balloons (alveoli) stretch out and break.
- The airway walls thicken and scar.
This combination creates a chronic obstructive lung disease. Air gets in, but it traps inside the chest. You exhale less, so each breath feels shallow.
The common types of COPD
Experts describe two common types of COPD:
- Chronic bronchitis – long‑term inflammation in the bronchial tubes with heavy mucus.
- Chronic bronchitis is defined as daily productive cough for at least three months in two consecutive years.
- Emphysema – destruction of the air sacs that give the lung its surface area.
Most patients with chronic obstructive disease have a mix of emphysema and chronic bronchitis, not one or the other.
Typical COPD symptoms and early warning signs
Key symptoms of COPD and signs of COPD include:
- Chronic cough, sometimes called “smoker’s cough”
- Thick or colored mucus
- Shortness of breath during activities, then at rest in severe COPD
- Wheezing or noisy breathing
- Chest tightness
- Fatigue and reduced exercise tolerance
- Frequent chest infections or acute exacerbations of COPD
Clinicians sometimes see these features as “normal aging,” and that delays the diagnosis of COPD. That delay hurts, because COPD is a progressive disease. Untreated, COPD progresses from mild breathlessness on hills to breathlessness while dressing.
Early COPD symptoms can look subtle, but they tell a story. That story starts with what damaged the lung in the first place.
3. Primary causes of COPD: what starts the damage
Smoking: the main cause of COPD
If you want the single biggest answer to “What is the cause of COPD?”, here it is:
Smoking stands as the main cause of COPD worldwide.
Current and former smokers account for most COPD cases in high‑income countries. Studies across Europe and North America show that roughly three out of four cases of COPD relate directly to cigarette smoking or heavy secondhand exposure.
Why smoking drives COPD:
- Each puff carries thousands of chemicals deep into the lung.
- These chemicals trigger inflammation in COPD, damaging airway lining and air sacs.
- The lung responds with extra mucus and scarring.
- Over years, this reshapes the airway structure and reduces pulmonary function.
Because of this evidence, guidelines describe smoking as the biggest risk factor for COPD. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) and the Initiative for Chronic Obstructive Lung Disease both stress smoking cessation as the foundation of the management of chronic obstructive pulmonary disease.
Key point:
If you smoke and you want to prevent COPD or stop COPD getting worse, quitting smoking sits at the very top of the priority list.
Air pollution and occupational exposures
Smoking does not act alone.
In many low‑ and middle‑income countries, the epidemiology of COPD looks different. Men and women with no smoking history inhale smoke from cooking fires, dusty mines, or factory fumes for decades. They still develop COPD.
Important non‑smoking causes and risk factor for COPD include:
- Indoor biomass fuel – wood, dung, or crop residue burned for cooking or heating, especially in poorly ventilated homes.
- Outdoor air pollution – traffic exhaust, industrial emissions, wildfire smoke.
- Occupational exposures – dusts from coal, silica, flour, grain, cotton, and fumes from welding, chemicals, or diesel.
When you inhale these particles day after day, they injure the airways in the same way tobacco smoke does. The risk of COPD climbs with intensity and duration of exposure.
Research on miners and industrial workers shows higher rates of COPD even when they never smoked. That research changed how experts talk about the burden of COPD, because it shifted blame away from personal choices alone and toward workplace safety and clean air policy.
Genetic factors: when lungs start with less protection
Genetics explain a smaller, yet critical, share of the development of COPD.
The classic example is alpha‑1 antitrypsin deficiency. Alpha‑1 antitrypsin is a protein that protects lung tissue from enzymes that break down elastin. When the body produces defective or low amounts of this protein, the lung loses that protection.
People with severe alpha‑1 deficiency get COPD at a younger age, even with light or no smoking history. Many receive a diagnosis of COPD in their 30s or 40s.
Clinicians estimate that genetic causes account for a minority of COPD cases, but missing this diagnosis has real consequences. These patients benefit from specific therapy in addition to standard COPD treatments.
So far, we looked at primary causes in general. The next question usually hits hard: “Can you get COPD even if you never smoked?” The answer changes how we think about risk for everyone in the room.
4. What causes COPD in non‑smokers?
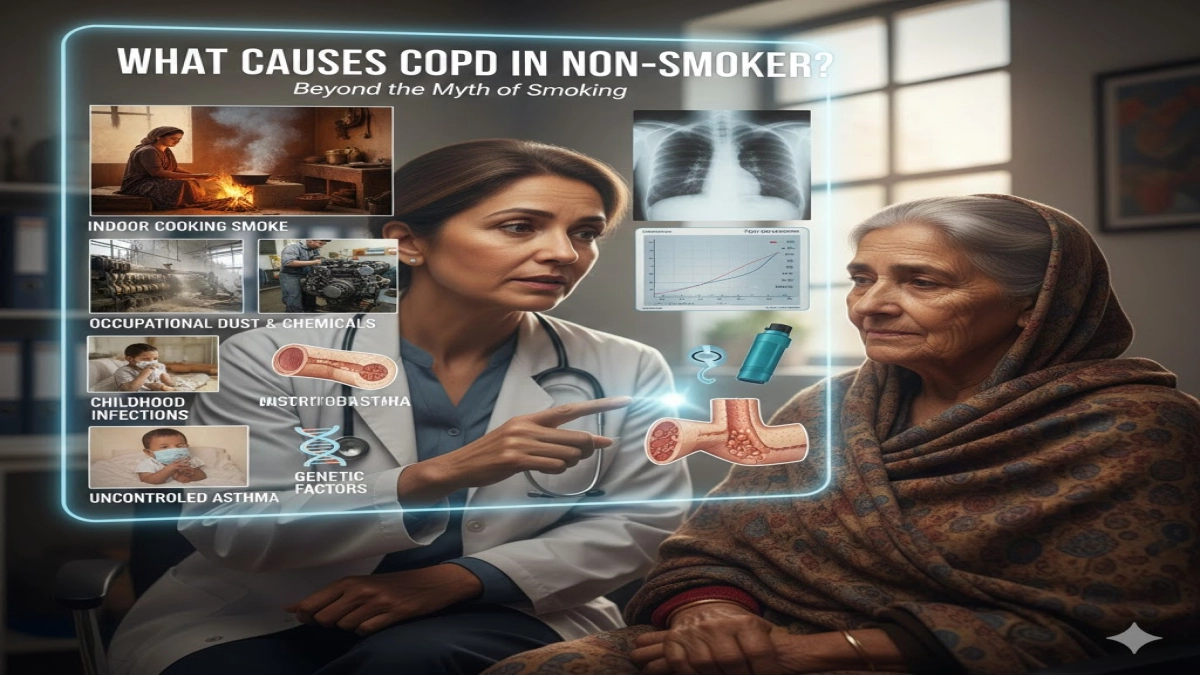
Non‑smoking related factors
Data from large population studies show that up to one third of COPD cases occur in people who never smoked. That number varies by country, but it always destroys the myth that COPD equals smoking only.
Key non‑smoking causes of COPD include:
- Long‑term exposure to indoor cooking smoke
- Occupational dust and chemicals
- Childhood respiratory infections that stunt lung growth
- Uncontrolled asthma
- Genetic conditions such as alpha‑1 antitrypsin deficiency
When I review COPD in primary care studies, one pattern repeats. Doctors see a woman in her 60s from a rural area with a chronic cough and breathlessness. She never touched cigarettes, but she cooked over an open fire for 40 years. A spirometry pulmonary function test confirms severe airflow obstruction.
On paper, she looks like every other patient with COPD. In reality, her story forces a deeper look at domestic air quality.
Environmental and occupational hazards
Think about your own day.
Do you work in:
- A textile mill with cotton or grain dust?
- A garage with diesel fumes?
- A salon with chemical aerosols?
These environments have strong links associated with COPD. Research shows COPD increases with cumulative exposure to these irritants. That exposure shapes your risk for COPD even if you never light a cigarette.
Many people with COPD often say, “I thought my mask protected me.” Thin paper masks help a little, yet they rarely block the tiny particles that damage the lung in a deep mine shaft or spray booth.
Asthma, interstitial lung disease, and COPD overlap
Two more lung problems intersect with COPD:
- Asthma and COPD – Long‑standing asthma with poor control can lead to structural airway changes that look like COPD on spirometry. Some patients develop an asthma–COPD overlap.
- COPD and interstitial lung disease – Certain workers, such as coal miners, show scarring patterns that combine COPD with interstitial changes.
These overlaps mean that COPD should be considered any time a mid‑life adult has persistent breathlessness and airflow limitation, even when the label on their chart still says “asthma” or “fibrosis.”
The causes change somewhat when you look beyond who develops COPD to what triggers sudden worsening. That brings us to the difference between long‑term causes and short‑term triggers.
5. Other causes of COPD besides smoking: secondhand smoke, air, and work
Air pollution as a driver of chronic lung damage
Air pollution does not just aggravate existing symptoms. Long‑term exposure contributes to the development of COPD even in non‑smokers.
Key points:
- Cities with high particulate pollution report higher rates of COPD and stronger COPD prevalence in population studies.
- People who grow up in polluted neighborhoods show reduced pulmonary function by early adulthood.
- Those with existing chronic lung disease experience more acute exacerbations of COPD when pollution levels spike.
In short, air pollution acts as both a cause and a trigger. That double role makes it important for both public health and personal action.
Secondhand smoke
You cannot smoke “for” someone else, yet you can damage their lungs.
Studies link secondhand smoke exposure in homes, bars, and workplaces to an increased risk of COPD and accelerated decline in lung function. Children who grow up with smokers show more childhood bronchitis and lower adult lung capacity.
For some never‑smokers, secondhand smoke acts as the main cause COPD alongside occupational dust or childhood infections.
Occupational exposures
You see this pattern in case series again and again:
- A worker spends 25 years in a grain silo, shipyard, or textile factory.
- He develops COPD symptoms in his 40s despite never smoking.
- Spirometry confirms a chronic obstructive lung disease picture.
Occupational lung researchers describe these as COPD associated with workplace inhalants. Industries with documented risk include:
- Mining and quarrying
- Construction and demolition
- Metal work and welding
- Textile, grain, and flour industries
- Chemical manufacturing
Workers in those fields carry a clear risk factor for COPD, especially when employers ignore protective equipment and ventilation standards.
You now know the slow drivers behind COPD. Next comes the question every person with established disease asks: “What sets off those bad weeks where breathing suddenly collapses?”
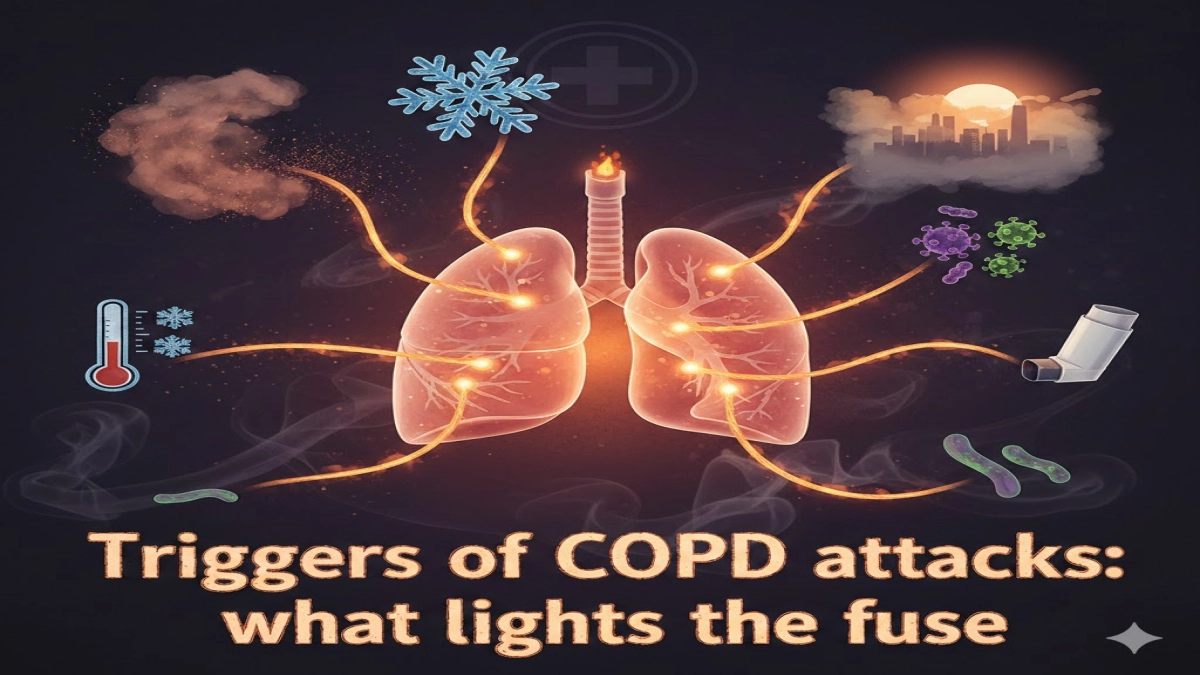
6. Triggers of COPD attacks: what lights the fuse
What is a COPD attack or exacerbation?
A COPD exacerbation or flare‑up means a sudden and sustained worsening of breathing symptoms that requires extra treatment such as steroids, antibiotics, or hospitalization.
Clinicians talk about acute exacerbations of COPD when:
- Breathlessness increases significantly.
- Cough and sputum increase or change color.
- Wheeze and chest tightness escalate.
- Oxygen levels drop.
These episodes matter because each major exacerbation speeds COPD progression, reduces long‑term quality of life, and raises mortality in COPD.
Common triggers of COPD flare‑ups
Common triggers include:
- Viral infections such as influenza, RSV, or common colds
- Bacterial bronchitis or pneumonia
- Sudden exposure to smoke, dust, or chemical fumes
- Cold, dry air or sharp temperature swings
- Very hot, humid weather
- Failure to take daily inhalers or stop them abruptly
Here is a typical scenario that appears in clinical audits:
A man with stable COPD manages everyday tasks with a maintenance inhaler. He runs out of medication before payday and stretches doses. A grandchild brings a winter virus home. Within days, his cough and breathlessness jump. He lands in hospital with an acute COPD flare.
The virus acted as the spark, but the missing inhaler primed his lungs.
Seasonal and weather‑related factors
In many regions, hospitals see a clear seasonal spike in COPD cases:
- Winter brings viral infections and cold air.
- Wildfire season brings smoke that lingers for weeks.
- Heat waves trap smog over cities.
Each pattern leads to clusters of acute exacerbations of COPD that push COPD in primary care and emergency departments to the limit.
You reduce risk dramatically when you understand which of these exposures matter most in your own life and how to create a personal action plan for them.
7. Causes of COPD exacerbation: deeper look
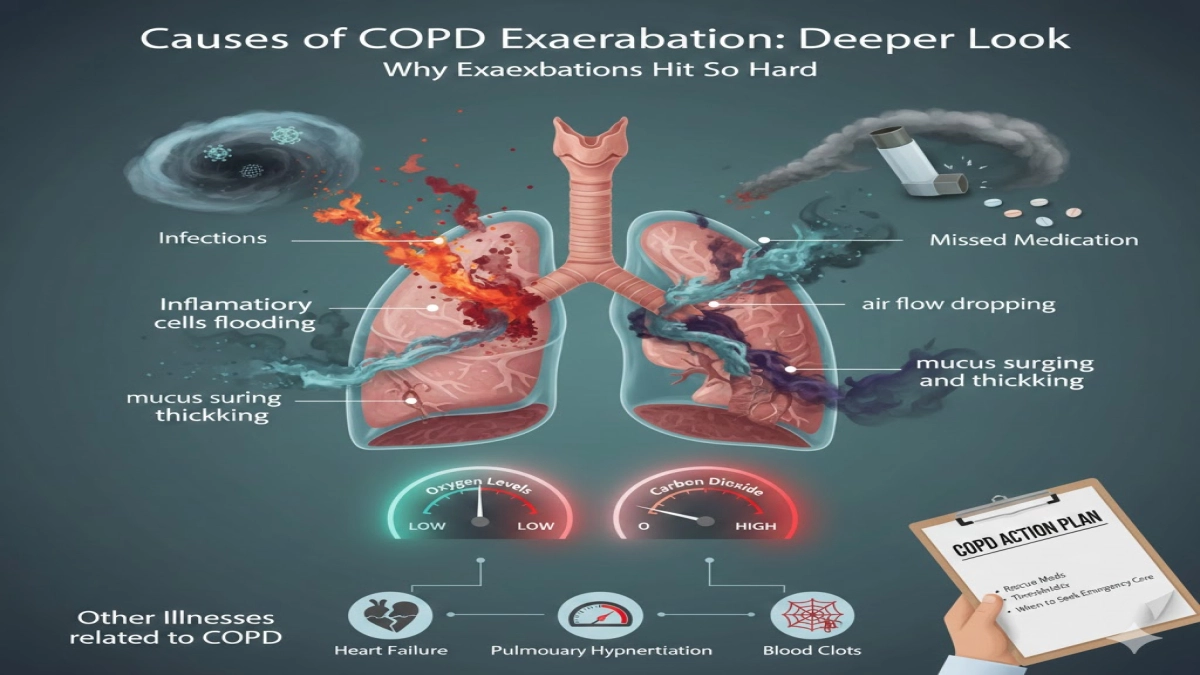
Why exacerbations hit so hard
A stable patient with COPD lives with chronic baseline inflammation and narrowed airways. When a trigger hits, several things happen:
- Inflammatory cells flood into the airways.
- Mucus production surges and thickens.
- Airflow drops further, especially in already damaged areas.
- Oxygen levels fall and carbon dioxide builds up.
This picture defines a feature of COPD that separates it from simple bronchitis: even when the infection clears, the underlying obstruction remains.
Main factors that drive exacerbations
Key causes of exacerbations include:
- Infections
- Respiratory viruses account for a large share of moderate and severe exacerbations.
- Bacterial infections contribute to sputum change and more serious flares that require antibiotics.
- Environmental irritants
- Short, intense exposure to smoke, dust, or chemicals flips someone from people with stable COPD into an emergency case.
- Missed or incorrect medication use
- Skipping maintenance inhalers
- Poor inhaler technique
- Stopping inhaled corticosteroids without a plan
- Other illnesses related to COPD
- Heart failure, pulmonary hypertension, or blood clots sometimes masquerade as a COPD flare.
- These conditions stay strongly related to COPD in advanced disease and contribute to COPD are more likely to die during hospital admissions.
I strongly recommend that every person with moderate to severe COPD keep a written action plan agreed with their clinician. That plan spells out thresholds for starting rescue medications and when to seek emergency care.
You now know what sparks the major attacks. Let us separate that from gentler “bad days,” or flare‑ups, which still deserve attention.
8. Triggers of COPD flare‑ups: bad days versus baseline
Flare‑ups versus regular symptoms
Daily symptoms in people with COPD can shift slightly with exertion, mood, or weather. A flare‑up goes beyond that. You notice:
- Extra breathlessness when climbing the same stairs
- More wheeze in the evening
- Thicker sputum
- More rescue inhaler use than usual
A flare‑up does not always meet the strict criteria of a full COPD exacerbation, yet it signals stress on the lungs.
Frequent minor flare‑ups predict major attacks. That makes them crucial early warning signs.
Common triggers for COPD flare‑ups
Frequent triggers include:
- Visiting a smoky bar or a home where people smoke
- Attending a barbecue or bonfire
- Cleaning dusty attics or basements
- Strong fragrances, air fresheners, or cleaning sprays
- Skipping regular exercise or pulmonary rehabilitation sessions
- Poor sleep and high stress
Think of a flare‑up as your lungs saying, “That exposure pushed me beyond my current capacity.”
When people with COPD also live with anxiety or depression, flare‑ups feel even worse and lead to more emergency visits. Mental health support forms an under‑appreciated part of the management of COPD.
Why recognizing triggers matters
Research on acute exacerbations of COPD shows that prevention yields more benefit than treating severe attacks alone. You win that prevention battle in your living room, workplace, and daily routines.
Pause and ask yourself:
- Which of these triggers hit my life weekly?
- Which can I remove, reduce, or protect myself against this month?
Once you know that, you can tailor the rest of your prevention and COPD treatments strategy.
9. Prevention and management strategies: changing the trajectory

COPD specialists agree on one core fact:
COPD is largely preventable and treatable, even though current science has no complete cure for COPD.
1. Stop smoking and avoid smoke exposure
For smokers, the best way to prevent COPD and slow COPD progression is clear:
- Set a quit date.
- Combine behavioral support with medication such as nicotine replacement, varenicline, or bupropion.
- Remove cigarettes, lighters, and ashtrays from your environment.
Research shows that quitting smoking:
- Slows the rate of lung function decline
- Reduces acute exacerbations of COPD
- Lowers mortality in COPD
- Improves overall quality of life
For non‑smokers, protect yourself from secondhand smoke. Set clear boundaries in your home and car. Choose smoke‑free venues.
2. Clean up the air around you
You cannot control city‑wide pollution alone, yet you can reduce your personal exposure:
- Use clean cooking fuels or improved stoves when possible.
- Ventilate kitchens and workshops.
- Wear proper respirators in dusty or fume‑heavy jobs.
- Check daily air quality reports and stay indoors or mask up on high‑pollution days.
These steps reduce the risk of COPD for you and your family and ease symptoms for people with COPD who already carry lung damage.
3. Get the right diagnosis with pulmonary function testing
Too many patients with chronic obstructive disease carry labels like “recurrent bronchitis” or “just asthma” for years.
To diagnose COPD correctly, doctors need a pulmonary function test (spirometry). This test:
- Measures how much air you blow out in one second (FEV1).
- Compares it to the total air you exhale (FVC).
- Confirms persistent airflow limitation.
Spirometry gives an objective diagnosis of COPD and helps stage disease severity. That staging shapes the management of chronic obstructive pulmonary disease for that person.
If you live with common symptoms of COPD such as chronic cough, breathlessness, or mucus and you have any history of COPD risk factors (smoking, biomass, dust), ask your clinician for spirometry.
4. Use evidence‑based COPD treatments
Modern COPD treatments aim to:
- Relieve daily symptoms
- Prevent exacerbations
- Slow structural damage
- Improve exercise capacity and quality of life
Main tools include:
- Inhaled bronchodilators – Long‑acting beta‑agonists (LABA) and long‑acting muscarinic antagonists (LAMA).
- Inhaled corticosteroids – For selected COPD patients with frequent exacerbations or asthma overlap.
- Combination inhalers – LABA/LAMA or LABA/ICS or triple therapy.
- Oxygen therapy – For advanced disease with resting hypoxemia.
- Pulmonary hypertension management when present.
Treating COPD works best when patients:
- Learn correct inhaler technique.
- Use maintenance inhalers every day, not just on bad days.
- Follow an agreed management of COPD plan during exacerbations.
Guidelines such as GOLD update treatment algorithms regularly. For example, the GOLD COPD May 2024 update highlights symptom burden and exacerbation history as central to treatment decisions.
5. Join a pulmonary rehabilitation program
If I had to pick one underused tool that transforms life for people with COPD, it would be pulmonary rehabilitation.
A structured pulmonary rehabilitation program usually includes:
- Supervised exercise training
- Breathing techniques and energy‑saving strategies
- Education about inhaler use and management of chronic respiratory symptoms
- Nutrition advice and mental health support
Research shows that pulmonary rehabilitation:
- Improves exercise tolerance
- Reduces breathlessness
- Cuts hospital admissions for acute exacerbations of COPD
- Lifts mood and overall quality of life
People who complete rehab describe a shift from “I can barely walk to the mailbox” to “I can shop for groceries again.” For people living with COPD, that change equals independence.
6. Monitor and manage comorbidities
COPD rarely appears alone. It frequently comes with:
- Heart disease
- Pulmonary hypertension
- Osteoporosis
- Anxiety and depression
- Metabolic syndrome
These conditions stay strongly associated with COPD and raise the risk of COPD worse outcomes, including mortality in COPD.
Regular check‑ups help your healthcare team track weight, bone health, mood, and cardiovascular status while they manage your lungs.
7. Vaccinations and infection prevention
Because infections trigger many acute exacerbations of COPD, every patient with COPD should:
- Receive annual influenza vaccination
- Stay up to date with pneumococcal and Covid‑19 vaccines
- Practice hand hygiene and avoid close contact with sick contacts when possible
These simple steps reduce COPD disease burden on both individuals and health systems.
8. Personal action plan for flare‑ups
Here is a basic framework many clinics use:
- Know your baseline
- Write down your usual breathlessness level and sputum amount.
- Define red flags
- Mark signs that indicate an early flare, such as needing your rescue inhaler more than three times a day or waking at night short of breath.
- Agree on rescue steps
- Short‑course steroids and antibiotics when appropriate
- When to call the clinic
- When to go to the emergency department
- Review after every exacerbation
- Adjust maintenance treatment.
- Revisit rehab and self‑management skills.
Clinicians who run COPD in primary care programs see clear benefits when patients carry a written plan and share it with family.
Because COPD is a long‑term condition and because COPD is permanent in terms of structural damage, smart day‑to‑day management becomes the lever that changes life expectancy and daily function.
10. Bringing it together: causes, triggers, and real control
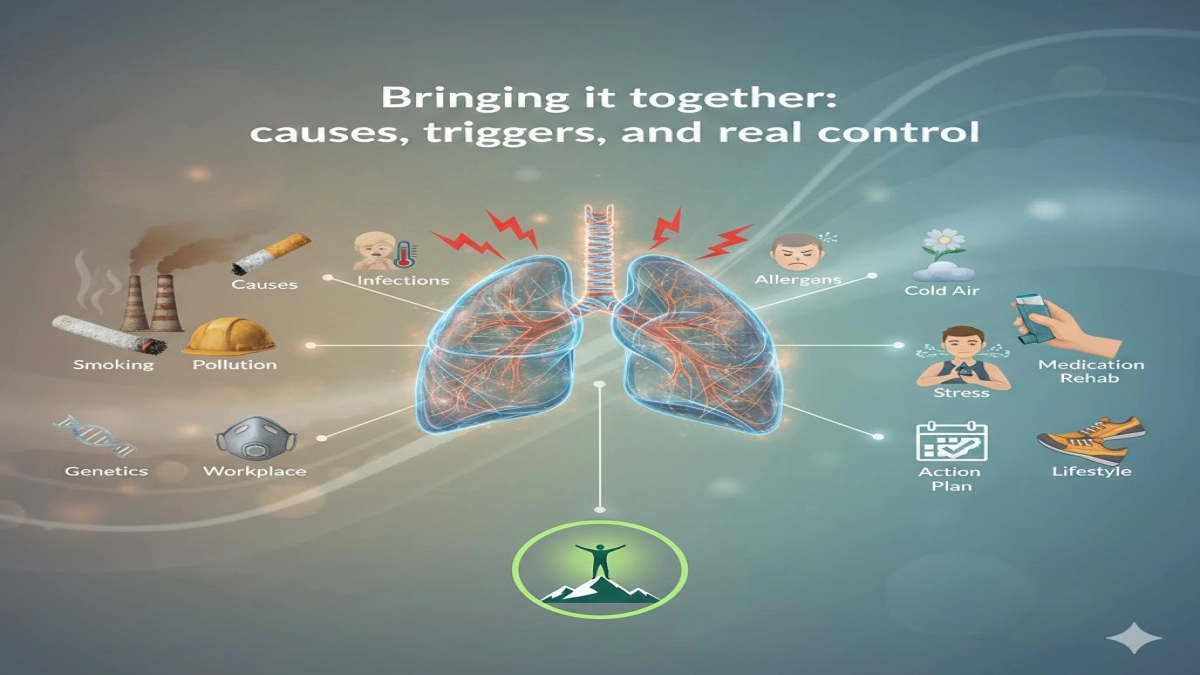
Let us connect the pieces.
- COPD is a lung condition grounded in chronic airway and alveolar damage.
- Smoking, polluted air, workplace exposures, and genetics stand as the common causes of COPD.
- These exposures interact with personal vulnerability to cause COPD, especially after midlife.
- Once established, COPD is a chronic condition that does not fully reverse, yet it responds strongly to smart treatment and behavior change.
- People with COPD also live with a higher risk of heart disease, pulmonary hypertension, depression, and other illnesses related to COPD.
- COPD often occurs silently over decades, so early attention to symptoms and causes beats waiting for a crisis.
- With the right prevention and management of chronic respiratory disease, people with COPD regain control over their activity level and social life.
When you understand these causes and triggers, you stop seeing COPD as an inevitable slide and start treating it as a condition you can influence every single day.
If you recognize yourself in the descriptions here, do not wait. Ask your clinician to:
- Review your exposure history
- Order a pulmonary function test
- Discuss a tailored plan covering smoking, air quality, inhalers, and pulmonary rehabilitation
Every month you act earlier improves the next decade of breathing.
People also ask: quick answers
1. Can you get COPD if you never smoked?
Yes. Up to one third of COPD cases occur in never-smokers due to air pollution, indoor cooking smoke, workplace dust, childhood lung infections, or genetic factors.
2. Is there a cure for COPD?
No. COPD damage is permanent, but early treatment can slow progression, reduce flare-ups, and improve daily life.
3. How do doctors diagnose COPD?
With spirometry. This breathing test measures airflow and confirms long-term obstruction after using a bronchodilator.
4. What is the difference between asthma and COPD?
Asthma is usually reversible and starts earlier. COPD causes fixed airflow blockage and typically appears after age 40.
5. Does COPD always get worse?
Not always. With early diagnosis, quitting smoking, proper inhalers, and rehab, many people stay stable for years.
6. What are the first signs of COPD?
Chronic cough, mucus, shortness of breath on exertion, and wheezing during colds or activity.
7. What is pulmonary rehabilitation?
A supervised program of exercise, breathing training, and education that improves stamina and reduces hospital visits.
8. Does COPD affect only the lungs?
No. COPD also raises the risk of heart disease, pulmonary hypertension, anxiety, depression, and bone loss.
References
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of COPD. 2024 report.
- World Health Organization. Chronic respiratory diseases: chronic obstructive pulmonary disease (COPD) fact sheet. Latest update before 2024.
- Centers for Disease Control and Prevention (CDC). COPD surveillance and COPD prevalence data for the United States.
Medical Disclaimer
Information on this website is for general education only. It is not medical advice.
The content on COPD.MEDLIFEGUIDE is written to help people understand COPD and other breathing conditions in a clear and simple way. It is not a substitute for professional medical care, diagnosis, or treatment.
Always talk to a licensed healthcare provider for personal medical concerns.
Do not ignore symptoms or delay getting help because of something you read on this site. If you think you may be having a medical emergency, call your local emergency number right away.